

Race-sex differences in the management of hyperlipidemia: the REasons for Geographic and Racial Differences in Stroke study
- PMID: 25891050
- PMCID: PMC4422177
- DOI: 10.1016/j.amepre.2014.10.025
Race-sex differences in the management of hyperlipidemia: the REasons for Geographic and Racial Differences in Stroke study
Abstract
Background: Lipid management is less aggressive in blacks than whites and women than men.
Purpose: To examine whether differences in lipid management for race-sex groups compared to white men are due to factors influencing health services utilization or physician prescribing patterns.
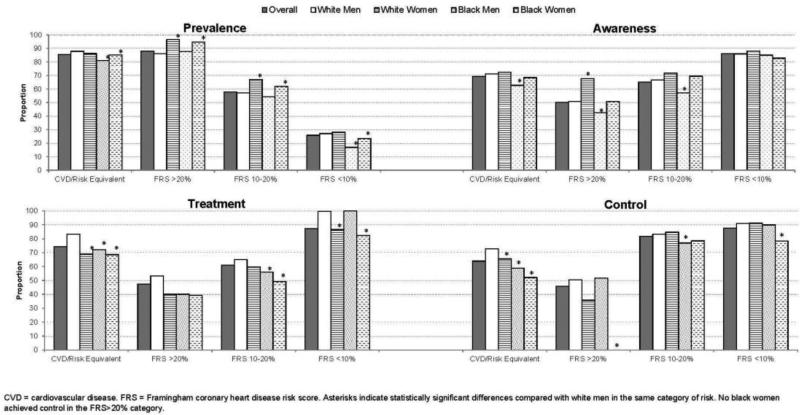
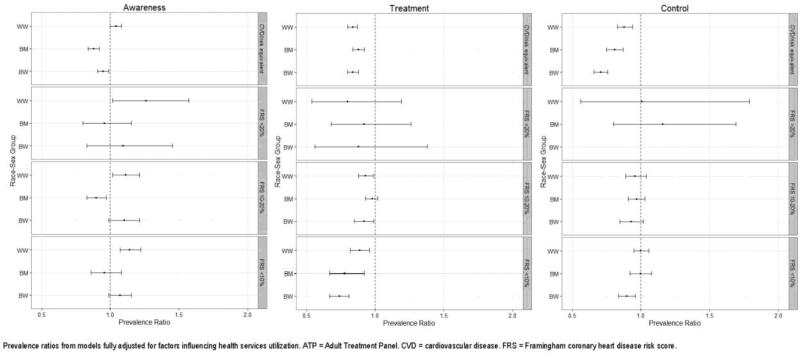
Methods: Because coronary heart disease (CHD) risk influences physician prescribing, Adult Treatment Panel III CHD risk categories were constructed using baseline data from REasons for Geographic And Racial Differences in Stroke study participants (recruited 2003-2007). Prevalence, awareness, treatment, and control of hyperlipidemia were examined for race-sex groups across CHD risk categories. Multivariable models conducted in 2013 estimated prevalence ratios adjusted for predisposing, enabling, and need factors influencing health services utilization.
Results: The analytic sample included 7,809 WM; 7,712 white women; 4,096 black men; and 6,594 black women. Except in the lowest risk group, black men were less aware of hyperlipidemia than others. A higher percentage of white men in the highest risk group was treated (83.2%) and controlled (72.8%) than others (treatment, 68.6%-72.1%; control, 52.2%-65.5%), with black women treated and controlled the least. These differences remained significant after adjustment for predisposing, enabling, and need factors. Stratified analyses demonstrated that treatment and control were lower for other race-sex groups relative to white men only in the highest risk category.
Conclusions: Hyperlipidemia was more aggressively treated and controlled among white men compared with white women, black men, and especially black women among those at highest risk for CHD. These differences were not attributable to factors influencing health services utilization.
Copyright © 2015 American Journal of Preventive Medicine. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- National Heart, Lung, and Blood Institute . Morbidity & Mortality: 2012 Chart Book on Cardiovascular, Lung, and Blood Diseases. NIH; Bethesda, MD: 2012.
-
- Safford MM, Brown TM, Muntner PM, et al. Association of race and sex with risk of incident acute coronary heart disease events. JAMA. 2012;308(17):1768–74. http://dx.doi.org/10.1001/jama.2012.14306. - DOI - PMC - PubMed
-
- Williams JE, Massing M, Rosamond WD, Sorlie PD, Tyroler HA. Racial disparities in CHD mortality from 1968-1992 in the state economic areas surrounding the ARIC study communities. Atherosclerosis Risk in Communities. Ann Epidemiol. 1999;9(8):472–480. http://dx.doi.org/10.1016/S1047-2797(99)00029-0. - DOI - PubMed
-
- Jones DW, Chambless LE, Folsom AR, et al. Risk factors for coronary heart disease in African Americans: the atherosclerosis risk in communities study, 1987-1997. Arch Intern Med. 2002;162(22):2565–71. http://dx.doi.org/10.1001/archinte.162.22.2565. - DOI - PubMed
-
- Mann D, Reynolds K, Smith D, Muntner P. Trends in statin use and low-density lipoprotein cholesterol levels among US adults: impact of the 2001 National Cholesterol Education Program guidelines. Ann Pharmacother. 2008;42(9):1208–15. http://dx.doi.org/10.1345/aph.1L181. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
