

Nivolumab and ipilimumab versus ipilimumab in untreated melanoma
- PMID: 25891304
- PMCID: PMC5744258
- DOI: 10.1056/NEJMoa1414428
Nivolumab and ipilimumab versus ipilimumab in untreated melanoma
Erratum in
-
Neoadjuvant PD-1 Blockade in Resectable Lung Cancer; Nivolumab and Ipilimumab in Advanced Melanoma; Overall Survival with Combined Nivolumab and Ipilimumab in Advanced Melanoma; Prolonged Survival in Stage III Melanoma with Ipilimumab Adjuvant Therapy; Combined Nivolumab and Ipilimumab or Monotherapy in Untreated Melanoma; Combined Nivolumab and Ipilimumab or Monotherapy in Untreated Melanoma; Nivolumab and Ipilimumab versus Ipilimumab in Untreated Melanoma; Rapid Eradication of a Bulky Melanoma Mass with One Dose of Immunotherapy; Genetic Basis for Clinical Response to CTLA-4 Blockade; Genetic Basis for Clinical Response to CTLA-4 Blockade in Melanoma; Nivolumab plus Ipilimumab in Advanced Melanoma; Safety and Tumor Responses with Lambrolizumab (Anti-PD-1) in Melanoma; Hepatotoxicity with Combination of Vemurafenib and Ipilimumab.N Engl J Med. 2018 Nov 29;379(22):2185. doi: 10.1056/NEJMx180040. Epub 2018 Nov 9. N Engl J Med. 2018. PMID: 31442371 No abstract available.
Abstract
Background: In a phase 1 dose-escalation study, combined inhibition of T-cell checkpoint pathways by nivolumab and ipilimumab was associated with a high rate of objective response, including complete responses, among patients with advanced melanoma.
Methods: In this double-blind study involving 142 patients with metastatic melanoma who had not previously received treatment, we randomly assigned patients in a 2:1 ratio to receive ipilimumab (3 mg per kilogram of body weight) combined with either nivolumab (1 mg per kilogram) or placebo once every 3 weeks for four doses, followed by nivolumab (3 mg per kilogram) or placebo every 2 weeks until the occurrence of disease progression or unacceptable toxic effects. The primary end point was the rate of investigator-assessed, confirmed objective response among patients with BRAF V600 wild-type tumors.
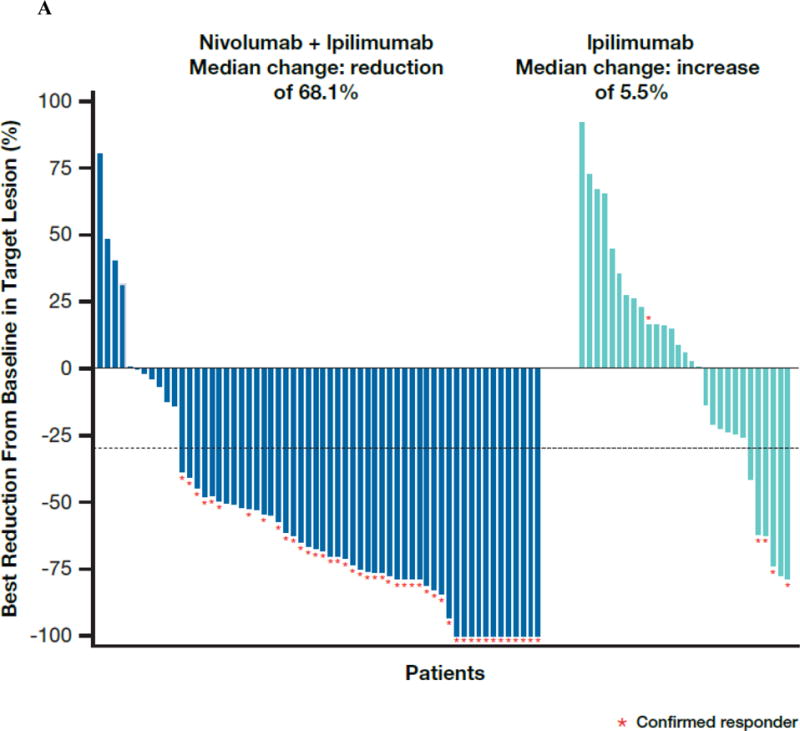
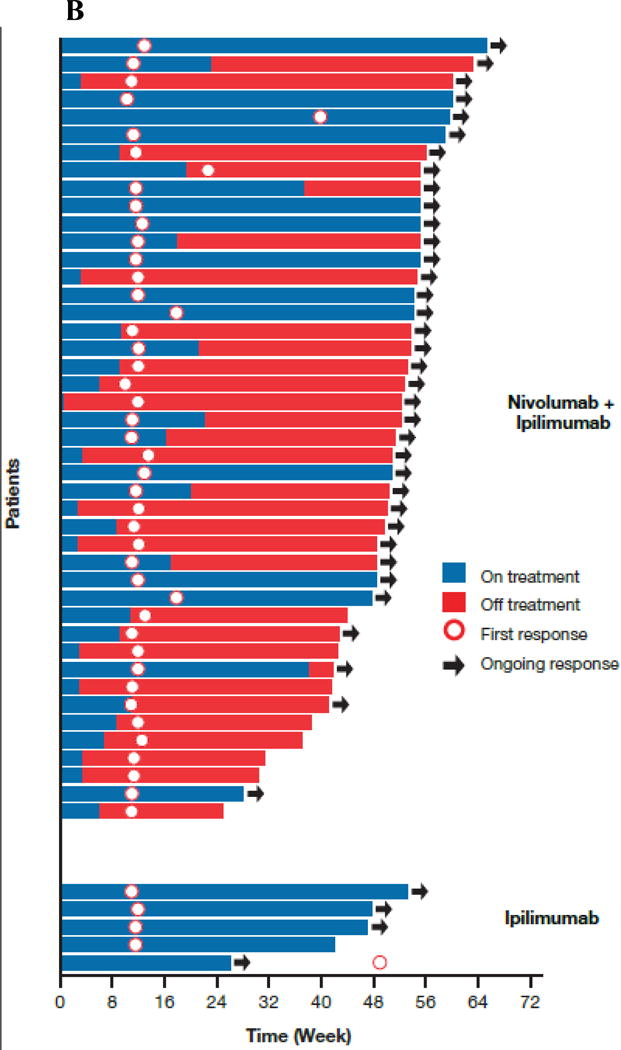
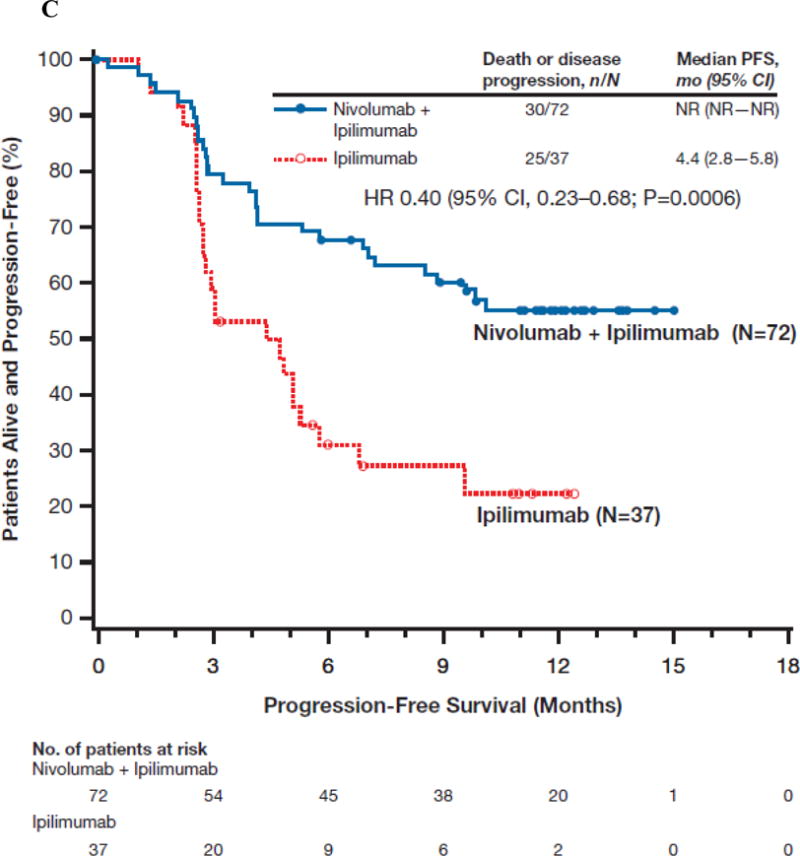
Results: Among patients with BRAF wild-type tumors, the rate of confirmed objective response was 61% (44 of 72 patients) in the group that received both ipilimumab and nivolumab (combination group) versus 11% (4 of 37 patients) in the group that received ipilimumab and placebo (ipilimumab-monotherapy group) (P<0.001), with complete responses reported in 16 patients (22%) in the combination group and no patients in the ipilimumab-monotherapy group. The median duration of response was not reached in either group. The median progression-free survival was not reached with the combination therapy and was 4.4 months with ipilimumab monotherapy (hazard ratio associated with combination therapy as compared with ipilimumab monotherapy for disease progression or death, 0.40; 95% confidence interval, 0.23 to 0.68; P<0.001). Similar results for response rate and progression-free survival were observed in 33 patients with BRAF mutation-positive tumors. Drug-related adverse events of grade 3 or 4 were reported in 54% of the patients who received the combination therapy as compared with 24% of the patients who received ipilimumab monotherapy. Select adverse events with potential immunologic causes were consistent with those in a phase 1 study, and most of these events resolved with immune-modulating medication.
Conclusions: The objective-response rate and the progression-free survival among patients with advanced melanoma who had not previously received treatment were significantly greater with nivolumab combined with ipilimumab than with ipilimumab monotherapy. Combination therapy had an acceptable safety profile. (Funded by Bristol-Myers Squibb; ClinicalTrials.gov number, NCT01927419.).
Figures
Comment in
-
Nivolumab + ipilimumab ups melanoma response.Cancer Discov. 2015 Jun;5(6):OF2. doi: 10.1158/2159-8290.CD-NB2015-058. Epub 2015 Apr 21. Cancer Discov. 2015. PMID: 25898833
-
Immunotherapy: Combined immunotherapy--a new standard in metastatic melanoma?Nat Rev Clin Oncol. 2015 Aug;12(8):439-40. doi: 10.1038/nrclinonc.2015.118. Epub 2015 Jun 23. Nat Rev Clin Oncol. 2015. PMID: 26099985 No abstract available.
References
-
- Robert C, Thomas L, Bondarenko I, et al. Ipilimumab plus dacarbazine for previously untreated metastatic melanoma. N Engl J Med. 2011;364:2517–2526. - PubMed
-
- Larkin J, Ascierto PA, Dreno B, et al. Combined vemurafenib and cobimetinib in BRAF-mutated melanoma. N Engl J Med. 2014;371:1867–1876. - PubMed
-
- Long GV, Stroyakovsky D, Gogas H, et al. Combined BRAF and MEK inhibition versus BRAF inhibition alone in melanoma. N Engl J Med. 2014;371:1877–1888. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials