

Review
doi: 10.1038/nrn3898.
Astrocyte barriers to neurotoxic inflammation
Affiliations
- PMID: 25891508
- PMCID: PMC5253239
- DOI: 10.1038/nrn3898
Item in Clipboard
Review
Astrocyte barriers to neurotoxic inflammation
Nat Rev Neurosci.
2015 May.
Erratum in
- Nat Rev Neurosci. 2015 Jun;16(6):372
Abstract
Astrocytes form borders (glia limitans) that separate neural from non-neural tissue along perivascular spaces, meninges and tissue lesions in the CNS. Transgenic loss-of-function studies reveal that astrocyte borders and scars serve as functional barriers that restrict the entry of inflammatory cells into CNS parenchyma in health and disease. Astrocytes also have powerful pro-inflammatory potential. Thus, astrocytes are emerging as pivotal regulators of CNS inflammatory responses. This Review discusses evidence that astrocytes have crucial roles in attracting and restricting CNS inflammation, with important implications for diverse CNS disorders.
Conflict of interest statement
statement The author declares no competing financial interests.
Figures
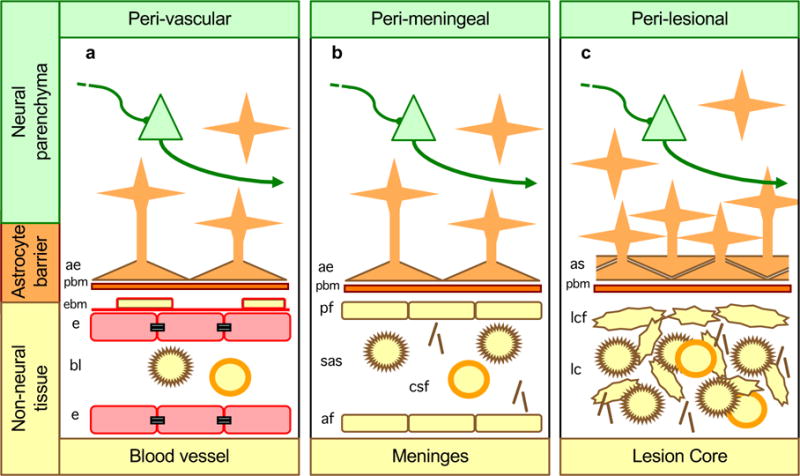
a| Along blood vessels, astrocyte endfeet and parenchymal basement membrane (PBM) present diverse molecular cues that constitute part of the multiple functional barriers, including endothelia with tight junctions and endothelial basement membrane (EBM), across which leukocytes must be actively recruited to pass from the bloodstream into CNS neural parenchyma, , . b| Abutting the meninges, astrocyte endfeet and parenchymal basement membranes present multiple molecular cues that restrict leukocytes in the subarachnoid space (SAS) from passing freely into CNS parenchyma. c| Surrounding tissue lesion cores (which are comprised of non-neural cells including leukocytes), astrocyte scars and parenchymal basement membrane are similar in appearance, organization and function to astrocyte borders lining non-neural cells along meninges and blood vessels, and similarly restrict the entry of leukocytes into adjacent CNS parenchyma.
|
| neuron |
| macrophage |
|
| T cell | ||
|
| astrocyte |
| collagen |
|
| astrocyte |
| tight junction |
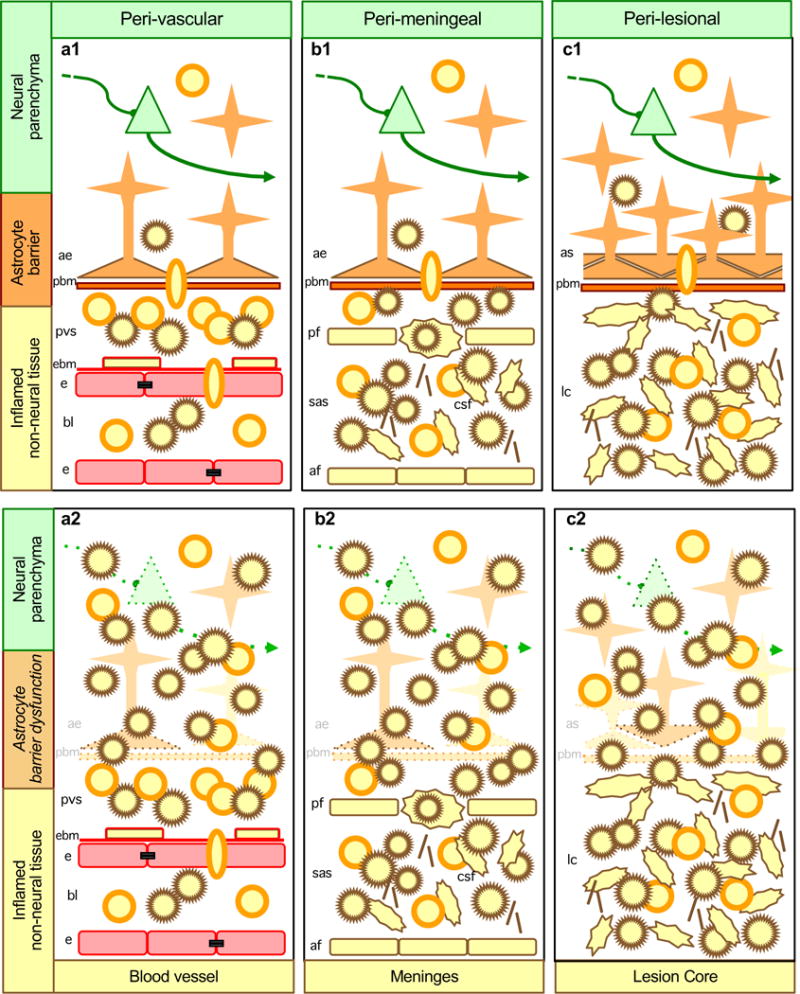
Aa| Along blood vessels, during autoimmune inflammation or certain infections, leukocytes are recruited across barriers of endothelia and endothelial basement membrane (EBM) and collect in perivascular spaces (PVS) but are restricted from passing freely into CNS parenchyma by molecular functional barriers presented by parenchymal basement membrane (PBM) and astrocyte endfeet. Ab| When astrocyte endfeet and parenchymal basement membrane are disrupted or rendered dysfunctional by experimental transgenic manipulations or by certain disease mechanisms, cytotoxic inflammation spreads into CNS parenchyma. Ba| Along meninges, during infections and autoimmune inflammation, leukocytes freely traffic and collect in the subarachnoid space (SAS) but are restricted from passing freely into CNS parenchyma by molecular functional barriers presented by parenchymal basement membrane and astrocyte endfeet. Bb| When astrocyte endfeet and parenchymal basement membrane are disrupted or rendered dysfunctional by experimental transgenic manipulations, cytotoxic inflammation spreads from the SAS into CNS parenchyma. Ca| At tissue lesions, leukocytes freely traffic and collect in non-neural lesion cores, but are largely excluded from adjacent viable CNS parenchyma when astrocytes scars and parenchymal basement membrane are intact and functional. Cb| When astrocyte scars and parenchymal basement membrane are disrupted or rendered dysfunctional by experimental transgenic manipulations, cytotoxic inflammation spreads from lesion cores into adjacent CNS parenchyma resulting in neural degeneration and increased lesion size.
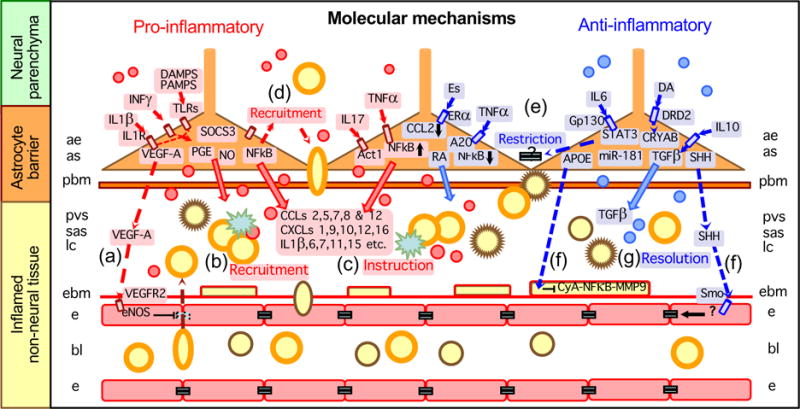
Entry of leukocytes into CNS parenchyma requires active recruitment across multiple cellular barriers, including an endothelial blood-brain barrier, endothelial (EBM) and parenchymal (PBM) basement membranes, and astrocytic functional barriers. Different molecules produced by astrocytes can take part in recruiting, restricting and instructing leukocytes in the CNS, as well as in promoting the resolution of inflammation over time. Thus, in response to different signaling mechanisms that are generated in different settings and at different times in relation to insult progression, astrocytes can in different contexts release molecules that (1) disrupt the blood-brain barrier by signaling to endothelia, (2) promote leukocyte extravasation into perivascular space (PVS), subarachnoid space (SAS) or lesion cores, (3) instruct leukocytes, (4) recruit leukocytes into CNS parenchyma, (5) restrict leukocyte entry into CNS parenchyma, or (6) repair the blood-brain barrier by signaling to pericytes, (7) promote resolution of inflammation or (8) repair the blood-brain barrier by signaling to endothelia. For molecular abbreviations see tables 1–3 and main text.
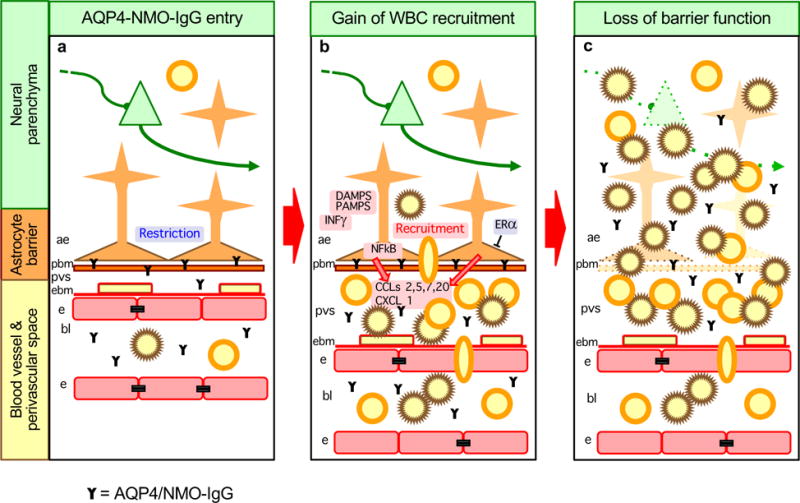
a| Stage 1. Sporadic or disease specific breaches of the blood-brain barrier lead to binding of AQP4/NMO-IgG to astrocyte membranes, which results in astrocyte functional changes. b| Stage 2. AQP4/NMO-IgG binding leads to astrocyte production of pro-inflammatory molecules and recruitment of leukocytes, initially into perivascular spaces (PVS). This process may be exacerbated by concomitant exposure to inflammatory mediators deriving from local or peripheral infections, such as DAMPs, PAMPs or INFγ. This process may be attenuated by estrogen related signaling mechanisms. c| Stage 3. Compliment-mediated astrocyte destruction leads to loss of astrocyte barrier functions and subsequent spread of neurotoxic inflammation into adjacent neural parenchyma.
References
-
- Ransohoff RM, Engelhardt B. The anatomical and cellular basis of immune surveillance in the central nervous system. Nat Rev Immunol. 2012;12:623–35. - PubMed
-
- Prinz M, Priller J. Microglia and brain macrophages in the molecular age: from origin to neuropsychiatric disease. Nat Rev Neurosci. 2014;15:300–12. - PubMed
-
- Barres BA. The mystery and magic of glia: a perspective on their roles in health and disease. Neuron. 2008;60:430–440. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
