

Detection of inflammatory sacroiliitis in children with magnetic resonance imaging: is gadolinium contrast enhancement necessary?
- PMID: 25892309
- PMCID: PMC4526191
- DOI: 10.1002/art.39159
Detection of inflammatory sacroiliitis in children with magnetic resonance imaging: is gadolinium contrast enhancement necessary?
Abstract
Objective: In adults, gadolinium contrast enhancement does not add incremental value to fluid-sensitive sequences for evaluation of bone marrow edema. This study was undertaken to determine if magnetic resonance imaging (MRI) contrast is necessary to assess lesions consistent with inflammatory sacroiliitis in children.
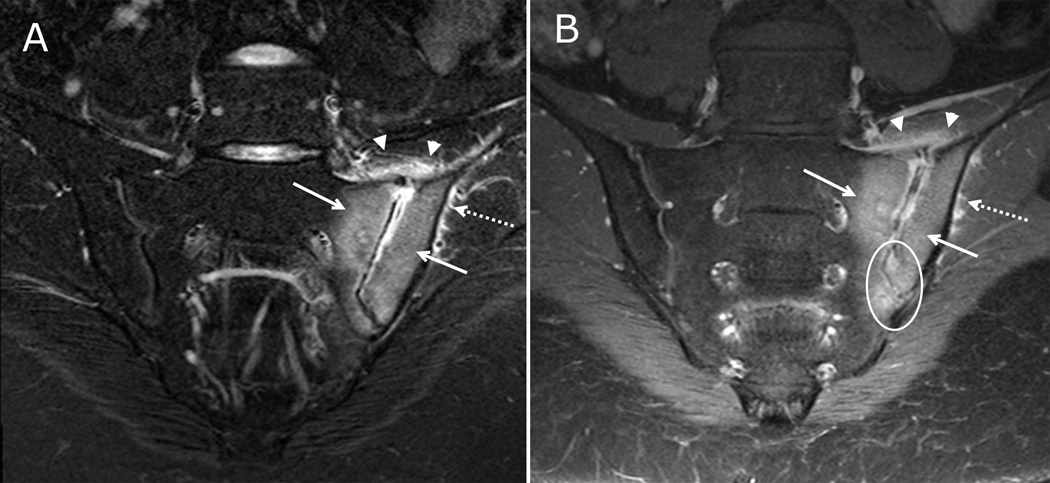
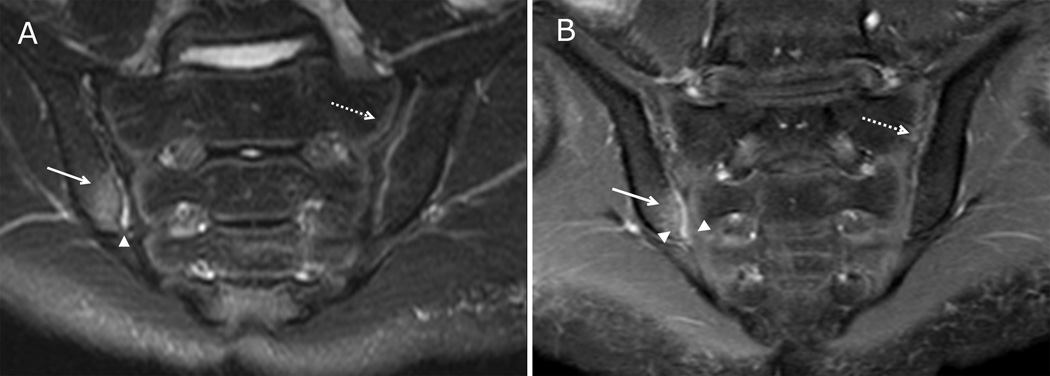
Methods: Patients with clinically suspected or diagnosed juvenile spondyloarthritis (SpA) underwent pelvic MRI consisting of multiplanar fluid-sensitive and postgadolinium T1-weighted fat-saturated sequences including dedicated sacral imaging. Three radiologists independently evaluated the fluid-sensitive sequences, and later, the complete study (including postcontrast images). With postcontrast imaging as the reference standard, we calculated the test properties of fluid-sensitive sequences for depiction of acute and chronic findings consistent with sacroiliitis.
Results: The 51 patients had a median age of 15 years, and 57% were male. Nineteen patients (22 joints) were diagnosed as having sacroiliitis based on postcontrast imaging, and none had synovitis in the absence of bone marrow edema. All 22 joints demonstrated bone marrow edema on both fluid-sensitive and postgadolinium T1-weighted fat-saturated sequences. Eighteen percent of joints with sacroiliitis had capsulitis, which was observed on both noncontrast and postcontrast imaging. Fifty-nine percent of joints with sacroiliitis had synovitis on postcontrast imaging. Sensitivity, specificity, positive predictive value, and negative predictive value of fluid-sensitive sequences for the detection of acute inflammatory lesions consistent with sacroiliitis using postgadolinium imaging as the reference standard were excellent. Interrater reliability was substantial for all parameters.
Conclusion: Our findings indicate that fluid-sensitive sequences are sufficient to detect acute and chronic lesions consistent with inflammatory sacroiliitis in children.
© 2015, American College of Rheumatology.
Figures
Comment in
-
Low Back Pain in Adolescents With Inflammatory Arthritis Can Be Due to Lumbar Spine Apophyseal Joint Inflammation, and This Requires Contrast Enhancement for Adequate Assessment: Comment on the Article by Weiss et al.Arthritis Rheumatol. 2016 Jan;68(1):263. doi: 10.1002/art.39452. Arthritis Rheumatol. 2016. PMID: 26474090 No abstract available.
-
Reply.Arthritis Rheumatol. 2016 Jan;68(1):263-4. doi: 10.1002/art.39456. Arthritis Rheumatol. 2016. PMID: 26474419 Free PMC article. No abstract available.
References
-
- Sieper J, Rudwaleit M, Baraliakos X, Brandt J, Braun J, Burgos-Vargas R, et al. The Assessment of SpondyloArthritis international Society (ASAS) handbook: a guide to assess spondyloarthritis. Ann Rheum Dis. 2009;68(Suppl 2):ii1–ii44. - PubMed
-
- de Hooge M, van den Berg R, Navarro-Compan V, van Gaalen F, van der Heijde D, Huizinga T, et al. Magnetic resonance imaging of the sacroiliac joints in the early detection of spondyloarthritis: no added value of gadolinium compared with short tau inversion recovery sequence. Rheumatology. 2013;52(7):1220–1224. - PubMed
-
- Tuite MJ. Sacroiliac joint imaging. Semin Musculoskelet Radiol. 2008;12(1):72–82. - PubMed
-
- Puhakka KB, Jurik AG, Egund N, Schiottz-Christensen B, Stengaard-Pedersen K, van Overeem Hansen G, et al. Imaging of sacroiliitis in early seronegative spondylarthropathy. Assessment of abnormalities by MR in comparison with radiography and CT. Acta Radiol. 2003;44(2):218–229. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
