

Fractures on bisphosphonates in osteoporosis pseudoglioma syndrome (OPPG): pQCT shows poor bone density and structure
- PMID: 25892485
- PMCID: PMC4480984
- DOI: 10.1016/j.bone.2015.04.007
Fractures on bisphosphonates in osteoporosis pseudoglioma syndrome (OPPG): pQCT shows poor bone density and structure
Abstract
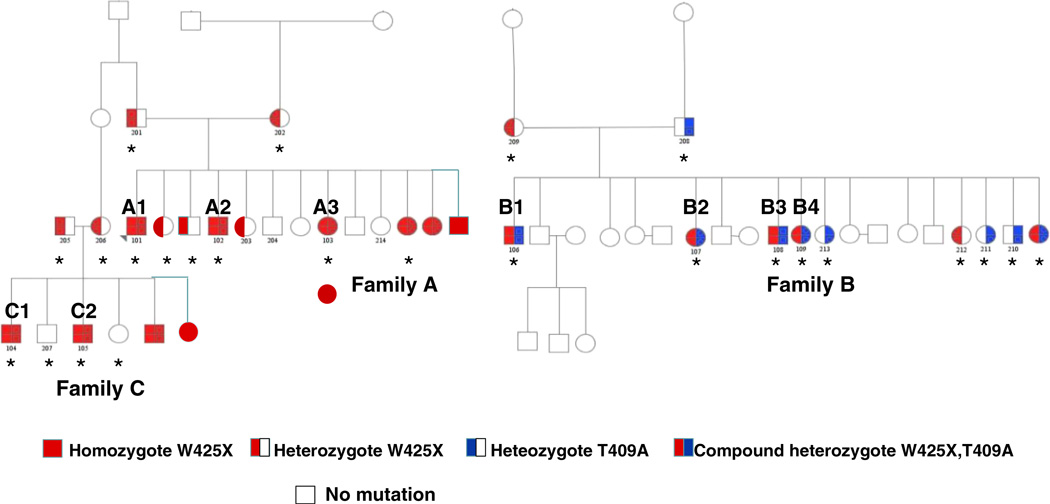
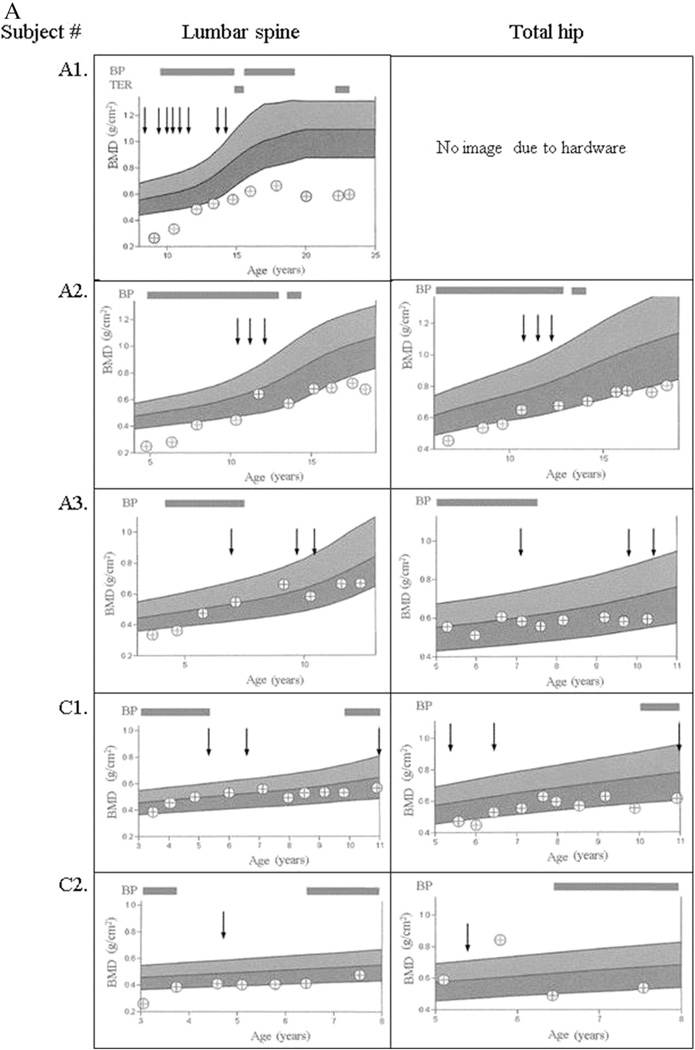
Osteoporosis pseudoglioma syndrome (OPPG) is a rare autosomal recessive disorder of childhood osteoporosis and blindness due to inactivating mutations in LDL receptor-like protein 5 (LRP5). We and others have reported improvement in areal bone mineral density (aBMD) by DXA in OPPG on short term bisphosphonates. Long-term data on bisphosphonate use in OPPG and measures of volumetric BMD (vBMD) and cortical structure are not available. In addition, no long-term DXA data on untreated OPPG is available. The aims of this study were to: (1) record low trauma fractures and longitudinal aBMD by DXA in 5 OPPG patients on chronic bisphosphonate treatment, and in 4 OPPG patients never treated (2) to perform tibia peripheral quantitative CT (pQCT) to evaluate volumetric bone mineral density (vBMD), cortical structure and calf muscle area in 6 OPPG patients and 14 unaffected first degree family members. pQCT results were converted to sex-specific Z-scores for age and adjusted for tibia length based on data in >700 reference participants. We observed 4 fractures (3 femoral shafts) in 3 OPPG patients while on bisphosphonates, after each achieved significant improvement in aBMD. OPPG participants had significantly lower mean trabecular vBMD (-1.51 vs. 0.17, p = 0.002), cortical area (-2.36 vs. 0.37; p < 0.001) and periosteal circumference (-1.86 vs. -0.31, p = 0.001) Z-scores, compared with unaffected participants and had a trend toward lower muscle area Z-score (-0.69 vs. 0.47, p = 0.12). These data demonstrate substantial bone fragility despite improvements in aBMD. The pQCT data provide insight into the fragility with substantial deficits in trabecular vBMD and cortical dimensions, consistent with OPPG effects of bone formation. Treatment that improves bone quality is needed to reduce fractures in OPPG.
Keywords: Atypical femur fracture; Bone mineral density; OPPG; Osteoporosis pseudoglioma syndrome; pQCT.
Copyright © 2015 Elsevier Inc. All rights reserved.
Conflict of interest statement
All authors state that they have no conflicts of interest.
Figures



References
-
- Gong Y, Slee RB, Fukai N, Rawadi G, Roman-Roman S, Reginato AM, et al. Osteoporosis-Pseudoglioma Syndrome Collaborative Group. LDL receptor-related protein 5 (LRP5) affects bone accrual and eye development. Cell. 2001;107:513–523. - PubMed
-
- DePaepe A, Leroy JG, Nuytinck L, Meire F, Capoen J. Osteoporosis-pseudoglioma syndrome. Am J Med Genet. 1993;45:30–37. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
