

Thyroid function within the normal range and risk of coronary heart disease: an individual participant data analysis of 14 cohorts
- PMID: 25893284
- PMCID: PMC4732559
- DOI: 10.1001/jamainternmed.2015.0930
Thyroid function within the normal range and risk of coronary heart disease: an individual participant data analysis of 14 cohorts
Abstract
Importance: Some experts suggest that serum thyrotropin levels in the upper part of the current reference range should be considered abnormal, an approach that would reclassify many individuals as having mild hypothyroidism. Health hazards associated with such thyrotropin levels are poorly documented, but conflicting evidence suggests that thyrotropin levels in the upper part of the reference range may be associated with an increased risk of coronary heart disease (CHD).
Objective: To assess the association between differences in thyroid function within the reference range and CHD risk.
Design, setting, and participants: Individual participant data analysis of 14 cohorts with baseline examinations between July 1972 and April 2002 and with median follow-up ranging from 3.3 to 20.0 years. Participants included 55,412 individuals with serum thyrotropin levels of 0.45 to 4.49 mIU/L and no previously known thyroid or cardiovascular disease at baseline.
Exposures: Thyroid function as expressed by serum thyrotropin levels at baseline.
Main outcomes and measures: Hazard ratios (HRs) of CHD mortality and CHD events according to thyrotropin levels after adjustment for age, sex, and smoking status.
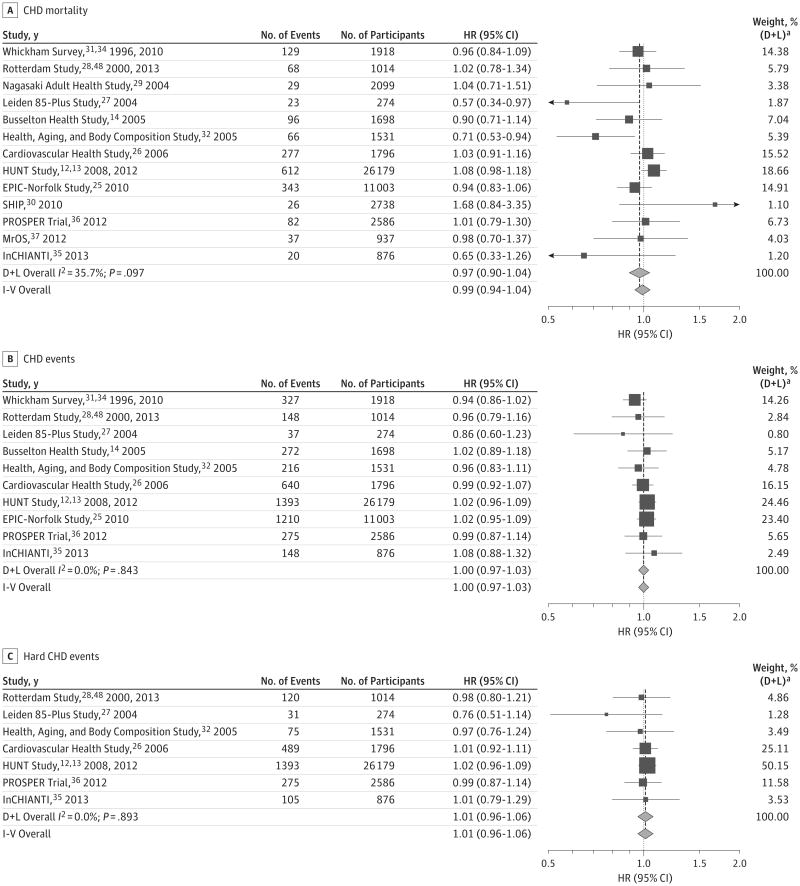
Results: Among 55,412 individuals, 1813 people (3.3%) died of CHD during 643,183 person-years of follow-up. In 10 cohorts with information on both nonfatal and fatal CHD events, 4666 of 48,875 individuals (9.5%) experienced a first-time CHD event during 533,408 person-years of follow-up. For each 1-mIU/L higher thyrotropin level, the HR was 0.97 (95% CI, 0.90-1.04) for CHD mortality and 1.00 (95% CI, 0.97-1.03) for a first-time CHD event. Similarly, in analyses by categories of thyrotropin, the HRs of CHD mortality (0.94 [95% CI, 0.74-1.20]) and CHD events (0.97 [95% CI, 0.83-1.13]) were similar among participants with the highest (3.50-4.49 mIU/L) compared with the lowest (0.45-1.49 mIU/L) thyrotropin levels. Subgroup analyses by sex and age group yielded similar results.
Conclusions and relevance: Thyrotropin levels within the reference range are not associated with risk of CHD events or CHD mortality. This finding suggests that differences in thyroid function within the population reference range do not influence the risk of CHD. Increased CHD risk does not appear to be a reason for lowering the upper thyrotropin reference limit.
Conflict of interest statement
Figures
References
-
- Cappola AR, Ladenson PW. Hypothyroidism and atherosclerosis. J Clin Endocrinol Metab. 2003;88(6):2438–2444. - PubMed
-
- Åsvold BO, Vatten LJ, Midthjell K, Bjøro T. Serum TSH within the reference range as a predictor of future hypothyroidism and hyperthyroidism: 11-year follow-up of the HUNT Study in Norway. J Clin Endocrinol Metab. 2012;97(1):93–99. - PubMed
-
- Spencer CA, Hollowell JG, Kazarosyan M, Braverman LE. National Health and Nutrition Examination Survey III thyroid-stimulating hormone (TSH)-thyroperoxidase antibody relationships demonstrate that TSH upper reference limits may be skewed by occult thyroid dysfunction. J Clin Endocrinol Metab. 2007;92(11):4236–4240. - PubMed
-
- Vanderpump MP, Tunbridge WM, French JM, et al. The incidence of thyroid disorders in the community: a twenty-year follow-up of the Whickham Survey. Clin Endocrinol (Oxf) 1995;43(1):55–68. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- N01 HC085080/HL/NHLBI NIH HHS/United States
- N01-AG-6-2101/AG/NIA NIH HHS/United States
- UL1 TR000128/TR/NCATS NIH HHS/United States
- R01-NR012459/NR/NINR NIH HHS/United States
- R01 NR012459/NR/NINR NIH HHS/United States
- HHSN268201200036C/HL/NHLBI NIH HHS/United States
- N01-AG-6-2106/AG/NIA NIH HHS/United States
- R01 AG032317/AG/NIA NIH HHS/United States
- WT_/Wellcome Trust/United Kingdom
- N01 AG062101/AG/NIA NIH HHS/United States
- U01 HL080295/HL/NHLBI NIH HHS/United States
- N01 HC085082/HL/NHLBI NIH HHS/United States
- K24 AR051895/AR/NIAMS NIH HHS/United States
- N01-AG-6-2103/AG/NIA NIH HHS/United States
- HHSN268200800007C/HL/NHLBI NIH HHS/United States
- N01 HC085086/HL/NHLBI NIH HHS/United States
- N01 HC085083/HL/NHLBI NIH HHS/United States
- DH_/Department of Health/United Kingdom
- AG-032317/AG/NIA NIH HHS/United States
- K24 AG042765/AG/NIA NIH HHS/United States
- G1000143/MRC_/Medical Research Council/United Kingdom
- U01 AG042124/AG/NIA NIH HHS/United States
- N01 AG062106/AG/NIA NIH HHS/United States
- U01 AG042145/AG/NIA NIH HHS/United States
- N01 HC055222/HL/NHLBI NIH HHS/United States
- G0401527/MRC_/Medical Research Council/United Kingdom
- N01 AG062103/AG/NIA NIH HHS/United States
- U01 AG042168/AG/NIA NIH HHS/United States
- N01 HC085079/HL/NHLBI NIH HHS/United States
- R10-AG028050/AG/NIA NIH HHS/United States
- U01 AG042140/AG/NIA NIH HHS/United States
- R01 HL080295/HL/NHLBI NIH HHS/United States
- R01 AG028050/AG/NIA NIH HHS/United States
- ImNIH/Intramural NIH HHS/United States
- HL080295/HL/NHLBI NIH HHS/United States
- U01 AG027810/AG/NIA NIH HHS/United States
- AG-023629/AG/NIA NIH HHS/United States
- R01 AG023629/AG/NIA NIH HHS/United States
- R56 AG023629/AG/NIA NIH HHS/United States
- U01 AG042143/AG/NIA NIH HHS/United States
- N01 HC085081/HL/NHLBI NIH HHS/United States
- U01 AG042139/AG/NIA NIH HHS/United States
- CRUK_/Cancer Research UK/United Kingdom
- U01 AR066160/AR/NIAMS NIH HHS/United States
- N01 HC55222/HC/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
