

Diagnosis and management of asthma in preschoolers: A Canadian Thoracic Society and Canadian Paediatric Society position paper
- PMID: 25893310
- PMCID: PMC4470545
- DOI: 10.1155/2015/101572
Diagnosis and management of asthma in preschoolers: A Canadian Thoracic Society and Canadian Paediatric Society position paper
Erratum in
-
Corrigendum.Paediatr Child Health. 2015 Oct;20(7):361. doi: 10.1093/pch/20.7.361. Paediatr Child Health. 2015. PMID: 26527376 Free PMC article. No abstract available.
-
Corrigendum Re: FM Ducharme, SD Dell, D Radhakrishnan, et al. Diagnosis and management of asthma in preschoolers: A Canadian Thoracic Society and Canadian Paediatric Society position paper. Can Respir J 2015;22(3):135-143.Can Respir J. 2015 Nov-Dec;22(6):348. doi: 10.1155/2015/761401. Can Respir J. 2015. PMID: 26641807 Free PMC article. No abstract available.
Abstract
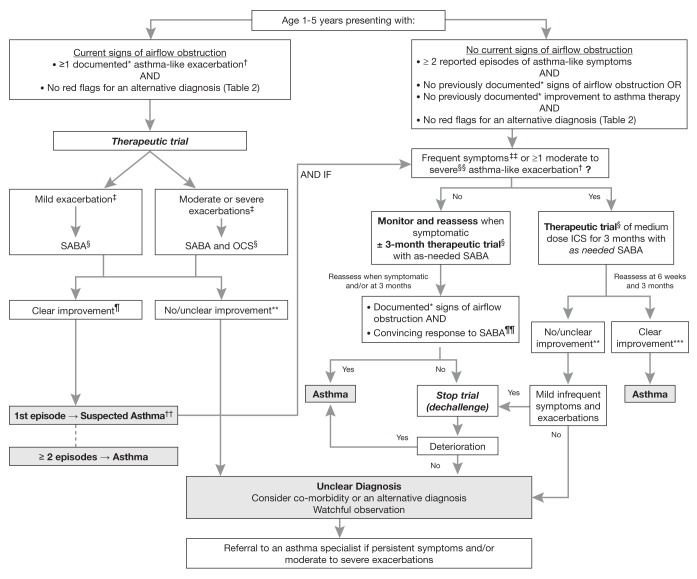
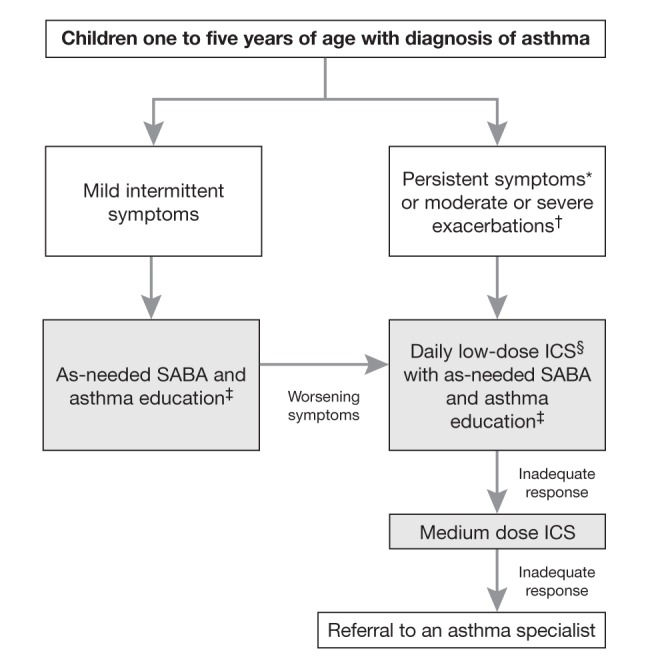
Asthma often starts before six years of age. However, there remains uncertainty as to when and how a preschool-age child with symptoms suggestive of asthma can be diagnosed with this condition. This delays treatment and contributes to both short- and long-term morbidity. Members of the Canadian Thoracic Society Asthma Clinical Assembly partnered with the Canadian Paediatric Society to develop a joint working group with the mandate to develop a position paper on the diagnosis and management of asthma in preschoolers. In the absence of lung function tests, the diagnosis of asthma should be considered in children one to five years of age with frequent (≥ 8 days/month) asthma-like symptoms or recurrent (≥ 2) exacerbations (episodes with asthma-like signs). The diagnosis requires the objective document of signs or convincing parent-reported symptoms of airflow obstruction (improvement in these signs or symptoms with asthma therapy), and no clinical suspicion of an alternative diagnosis. The characteristic feature of airflow obstruction is wheezing, commonly accompanied by difficulty breathing and cough. Reversibility with asthma medications is defined as direct observation of improvement with short-acting ß2-agonists (SABA) (with or without oral corticosteroids) by a trained health care practitioner during an acute exacerbation (preferred method). However, in children with no wheezing (or other signs of airflow obstruction) on presentation, reversibility may be determined by convincing parental report of a symptomatic response to a three-month therapeutic trial of a medium dose of inhaled corticosteroids with as-needed SABA (alternative method), or as-needed SABA alone (weaker alternative method). The authors provide key messages regarding in whom to consider the diagnosis, terms to be abandoned, when to refer to an asthma specialist and the initial management strategy. Finally, dissemination plans and priority areas for research are identified.
L’asthme fait souvent son apparition avant l’âge de six ans. Cependant, il subsiste des incertitudes relativement à quand et comment un enfant d’âge préscolaire ayant des symptômes de type asthmatique peut être diagnostiqué avec cette condition. Ceci retarde le traitement et contribue à la morbidité à court et à long terme. L’Assemblée clinique sur l’asthme de la Société canadienne de thoracologie s’est associée à la Société canadienne de pédiatrie pour créer un groupe de travail conjoint afin de préparer un document de principes sur le diagnostic et la prise en charge de l’asthme chez les enfants d’âge préscolaire.
En l’absence de mesures de la fonction pulmonaire, le diagnostic d’asthme devrait être envisagé chez les enfants de un à cinq ans ayant des symptômes de type asthmatique fréquents (≥8 jours/mois) ou des exacerbations récurrentes (≥2) (épisodes accompagnés de signes compatibles). Le diagnostic nécessite une documentation objective des signes cliniques ou un compte rendu parental convaincant de symptômes d’obstruction des voies respiratoires et de réversibilité de l’ obstruction (amélioration suite à un traitement pour l’asthme), ainsi que l’absence de suspicion clinique de tout autre diagnostic. La respiration sifflante, souvent accompagnée de difficultés respiratoires et de toux, est le signe cardinal de l’obstruction des voies respiratoires. La réversibilité à la suite de la prise de médicaments pour l’asthme se définie par l’observation directe par un professionnel de la santé compétent, d’une amélioration après l’administration de ß2-agonistes à courte durée d’action (BACA) (accompagnés ou non de corticostéroïdes par voie orale) pendant une exacerbation aigue (méthode diagnostique privilégiée). Cependant, chez les enfants qui n’ont pas à l’examen une respiration sifflante (ni d’autres signes d’obstruction des voies respiratoires), la réversibilité peut être déterminée par un compte rendu parental convaincant d’une réponse symptomatique à un essai thérapeutique de trois mois de corticostéroïdes inhalés, à dose moyenne, avec un BACA au besoin (méthode diagnostique alternative), ou avec seulement un BACA au besoin (méthode diagnostique alternative moins certaine) est recommandé. Les auteurs présentent des messages clés quant aux enfants chez lesquels on doit envisager le diagnostic, quant aux termes désuets à abandonner, quant aux situations pour lesquelles on doit orienter l’enfant vers un spécialiste de l’asthme et quant à la stratégie de prise en charge initiale. Enfin, ils décrivent la stratégie de diffusion de ces messages et identifient les domaines de recherche prioritaires.
Figures
Similar articles
-
Diagnosis and management of asthma in preschoolers: A Canadian Thoracic Society and Canadian Paediatric Society position paper.Paediatr Child Health. 2015 Oct;20(7):353-71. doi: 10.1093/pch/20.7.353. Paediatr Child Health. 2015. PMID: 26526095 Free PMC article.
-
Guidelines for the emergency management of asthma in adults. CAEP/CTS Asthma Advisory Committee. Canadian Association of Emergency Physicians and the Canadian Thoracic Society.CMAJ. 1996 Jul 1;155(1):25-37. CMAJ. 1996. PMID: 8673983 Free PMC article. Review.
-
Canadian Asthma Consensus Report, 1999. Canadian Asthma Consensus Group.CMAJ. 1999 Nov 30;161(11 Suppl):S1-61. CMAJ. 1999. PMID: 10906907 Free PMC article. Review.
-
Guideline for the management of chronic asthma in children--2000 update. Allergy Society of South Africa Working Group.S Afr Med J. 2000 May;90(5 Pt 2):524-8, 530, 532 passim. S Afr Med J. 2000. PMID: 10901828
-
Overcoming gaps in the management of asthma in older patients: new insights.Drugs Aging. 2005;22(12):1029-59. doi: 10.2165/00002512-200522120-00004. Drugs Aging. 2005. PMID: 16363886 Review.
Cited by
-
Biomarkers for Recurrent Wheezing and Asthma in Preschool Children.Allergy Asthma Immunol Res. 2019 Jan;11(1):16-28. doi: 10.4168/aair.2019.11.1.16. Allergy Asthma Immunol Res. 2019. PMID: 30479074 Free PMC article. Review.
-
Patterns of respiratory health services utilization from birth to 5 years of children who experienced adverse birth outcomes.PLoS One. 2021 Feb 19;16(2):e0247527. doi: 10.1371/journal.pone.0247527. eCollection 2021. PLoS One. 2021. PMID: 33606848 Free PMC article.
-
Effect of diagnosis delay on pulmonary function in children with asthma.Allergy Asthma Clin Immunol. 2022 Oct 19;18(1):92. doi: 10.1186/s13223-022-00731-w. Allergy Asthma Clin Immunol. 2022. PMID: 36261858 Free PMC article.
-
Neuropsychiatric adverse drug reactions in children initiated on montelukast in real-life practice.Eur Respir J. 2017 Aug 17;50(2):1700148. doi: 10.1183/13993003.00148-2017. Print 2017 Aug. Eur Respir J. 2017. PMID: 28818882
-
Physician agreement regarding the expansion of pharmacist professional activities in the management of patients with asthma.Int J Pharm Pract. 2017 Oct;25(5):335-342. doi: 10.1111/ijpp.12320. Epub 2016 Oct 24. Int J Pharm Pract. 2017. PMID: 27774739 Free PMC article.
References
-
- GINA Global Initiative for Asthma P Global strategy for asthma management and prevention. Global Initiative for Asthma 2014. < www.ginasthma.org/> (Accesssed May 2014).
-
- Castro-Rodriguez JA, Holberg CJ, Wright AL, Martinez FD. A clinical index to define risk of asthma in young children with recurrent wheezing. Am J Respir Crit Care Med. 2000;162:1403–6. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
