

Surgical Options and Locoregional Recurrence in Patients Diagnosed with Invasive Lobular Carcinoma of the Breast
- PMID: 25893416
- PMCID: PMC4801503
- DOI: 10.1245/s10434-015-4570-8
Surgical Options and Locoregional Recurrence in Patients Diagnosed with Invasive Lobular Carcinoma of the Breast
Abstract
Purpose: Recent consensus guidelines on margins for breast-conserving surgery (BCS) recommend the use of "no ink on tumor" as the standard for an adequate margin. The recommendations extend to invasive lobular carcinoma (ILC), but the data on this subset are limited. We reviewed our modern dataset on margin status with outcomes of ILC.
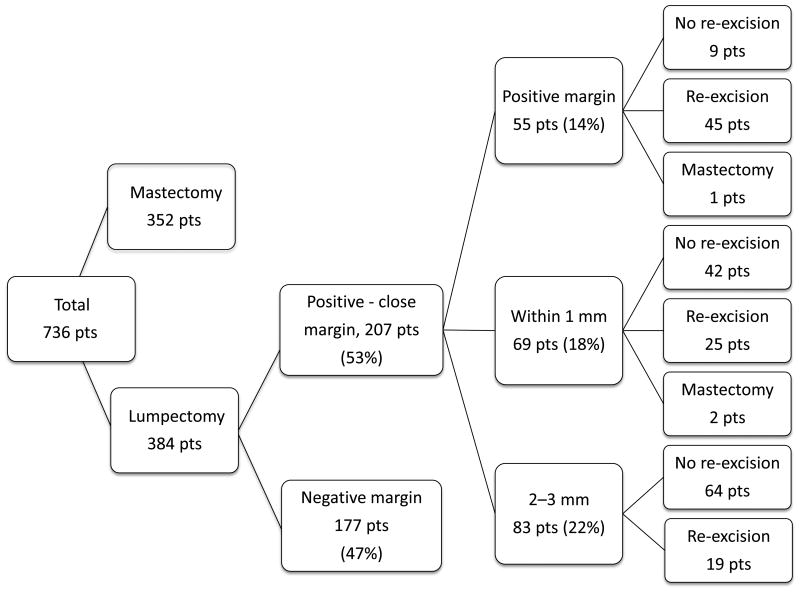
Methods: We performed a retrospective cohort study on 736 patients with a diagnosis of stage I-III ILC treated at our cancer center between May 1997 and December 2007. Clinicopathologic data were extracted from the Clinical Research Information Systems Database. Margin status was defined using the latest ASCO/ASTRO/SSO consensus guideline criteria.
Results: The initial surgery performed was mastectomy in 352 patients (48 %) and BCS in 384 patients (52 %). In multivariate analysis, tumor size and multifocality were significantly associated with high rates of mastectomy and positive surgical margins at initial BCS. After initial BCS, additional surgery was performed in 92 patients (24 %). During a 72-month median follow-up period, 12 (3.1 %) ipsilateral breast tumor recurrences (IBTR) and 5 (1.3 %) other locoregional recurrences (LRR) were observed. Patients with margins with ink on tumor who did not receive further surgery were found to have significantly increased LRR [odds ratio (OR) 5.5; p = 0.02] and IBTR (OR 8.5; p = 0.006), whereas patients with close margins (1-3 mm) and margins within 1 mm were not.
Conclusions: Our study supports the validity of using "no ink on tumor" as the standard for a negative margin for pure and mixed ILC treated with multimodality therapy.
Conflict of interest statement
Figures
References
-
- Li CI, Anderson BO, Daling JR, Moe RE. Trends in incidence rates of invasive lobular and ductal breast carcinoma. JAMA. 2003;289:1421–1424. - PubMed
-
- Yoder BJ, Wilkinson EJ, Massoll NA. Molecular and morphologic distinctions between infiltrating ductal and lobular carcinoma of the breast. Breast J. 2007;13:172–179. - PubMed
-
- Buchanan CL, Flynn LW, Murray MP, et al. Is pleomorphic lobular carcinoma really a distinct clinical entity? J Surg Oncol. 2008;98:314–317. - PubMed
-
- Jacobs M, Fan F, Tawfik O. Clinicopathologic and biomarker analysis of invasive pleomorphic lobular carcinoma as compared with invasive classic lobular carcinoma: An experience in our institution and review of the literature. Ann Diagn Pathol. 2012;16:185–189. - PubMed
-
- Iorfida M, Maiorano E, Orvieto E, et al. Invasive lobular breast cancer: subtypes and outcome. Breast Cancer Res Treat. 2012;133:713–23. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
