

Cost-effectiveness and population impact of statins for primary prevention in adults aged 75 years or older in the United States
- PMID: 25894023
- PMCID: PMC4476404
- DOI: 10.7326/M14-1430
Cost-effectiveness and population impact of statins for primary prevention in adults aged 75 years or older in the United States
Abstract
Background: Evidence to guide primary prevention in adults aged 75 years or older is limited.
Objective: To project the population impact and cost-effectiveness of statin therapy in adults aged 75 years or older.
Design: Forecasting study using the Cardiovascular Disease Policy Model, a Markov model.
Data sources: Trial, cohort, and nationally representative data sources.
Target population: U.S. adults aged 75 to 94 years.
Time horizon: 10 years.
Perspective: Health care system.
Intervention: Statins for primary prevention based on low-density lipoprotein cholesterol threshold of 4.91 mmol/L (190 mg/dL), 4.14 mmol/L (160 mg/dL), or 3.36 mmol/L (130 mg/dL); presence of diabetes; or 10-year risk score of at least 7.5%.
Outcome measures: Myocardial infarction (MI), coronary heart disease (CHD) death, disability-adjusted life-years, and costs.
Results of base-case analysis: All adults aged 75 years or older in the National Health and Nutrition Examination Survey have a 10-year risk score greater than 7.5%. If statins had no effect on functional limitation or cognitive impairment, all primary prevention strategies would prevent MIs and CHD deaths and be cost-effective. Treatment of all adults aged 75 to 94 years would result in 8 million additional users and prevent 105 000 (4.3%) incident MIs and 68 000 (2.3%) CHD deaths at an incremental cost per disability-adjusted life-year of $25 200.
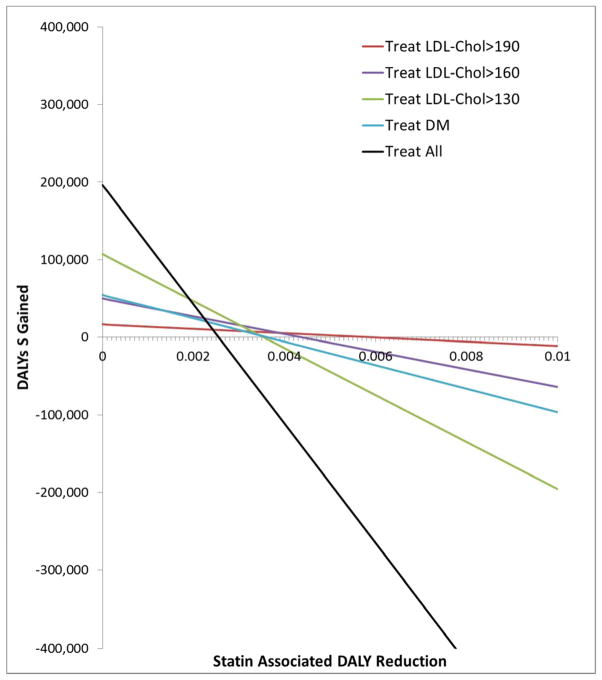
Results of sensitivity analysis: An increased relative risk for functional limitation or mild cognitive impairment of 1.10 to 1.29 could offset the cardiovascular benefits.
Limitation: Limited trial evidence targeting primary prevention in adults aged 75 years or older.
Conclusion: At effectiveness similar to that in trials, statins are projected to be cost-effective for primary prevention; however, even a small increase in geriatric-specific adverse effects could offset the cardiovascular benefit. Improved data on the potential benefits and harms of statins are needed to inform decision making.
Primary funding source: American Heart Association Western States Affiliate, National Institute on Aging, and the National Institute for Diabetes on Digestive and Kidney Diseases.
Figures
Comment in
-
Statins for Primary Prevention in Adults Aged 75 Years or Older.Ann Intern Med. 2015 Sep 15;163(6):481. doi: 10.7326/L15-5135. Ann Intern Med. 2015. PMID: 26370013 No abstract available.
-
Statins for Primary Prevention in Adults Aged 75 Years or Older.Ann Intern Med. 2015 Sep 15;163(6):481. doi: 10.7326/L15-5135-2. Ann Intern Med. 2015. PMID: 26370014 No abstract available.
-
Statins for Primary Prevention in Adults Aged 75 Years or Older.Ann Intern Med. 2015 Sep 15;163(6):482. doi: 10.7326/L15-5135-3. Ann Intern Med. 2015. PMID: 26370015 No abstract available.
Summary for patients in
-
Statins for primary prevention in older adults.Ann Intern Med. 2015 Apr 21;162(8):I-28. doi: 10.7326/P15-9012. Ann Intern Med. 2015. PMID: 25894041 No abstract available.
References
-
- Stone NJ, Robinson JG, Lichtenstein AH, et al. 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129(25 Suppl 2):S1–45. - PubMed
-
- AMDA. [Accessed April 22, 2014];Five Things Physicians and Patients Should Question. 2013 ( http://www.amda.com/tools/choosingwisely.cfm)
-
- Kronmal RA, Cain KC, Ye Z, et al. Total serum cholesterol levels and mortality risk as a function of age. A report based on the Framingham data. Arch Intern Med. 1993;153(9):1065–73. - PubMed
-
- Krumholz HM, Seeman TE, Merrill SS, et al. Lack of association between cholesterol and coronary heart disease mortality and morbidity and all-cause mortality in persons older than 70 years. JAMA. 1994;272(17):1335–40. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials