

Long-Term Once-Daily Tiotropium Respimat® Is Well Tolerated and Maintains Efficacy over 52 Weeks in Patients with Symptomatic Asthma in Japan: A Randomised, Placebo-Controlled Study
- PMID: 25894430
- PMCID: PMC4404354
- DOI: 10.1371/journal.pone.0124109
Long-Term Once-Daily Tiotropium Respimat® Is Well Tolerated and Maintains Efficacy over 52 Weeks in Patients with Symptomatic Asthma in Japan: A Randomised, Placebo-Controlled Study
Abstract
Background: This study assessed the long-term safety and efficacy of tiotropium Respimat, a long-acting inhaled anticholinergic bronchodilator, in asthma, added on to inhaled corticosteroids (ICS) with or without long-acting β2-agonist (LABA).
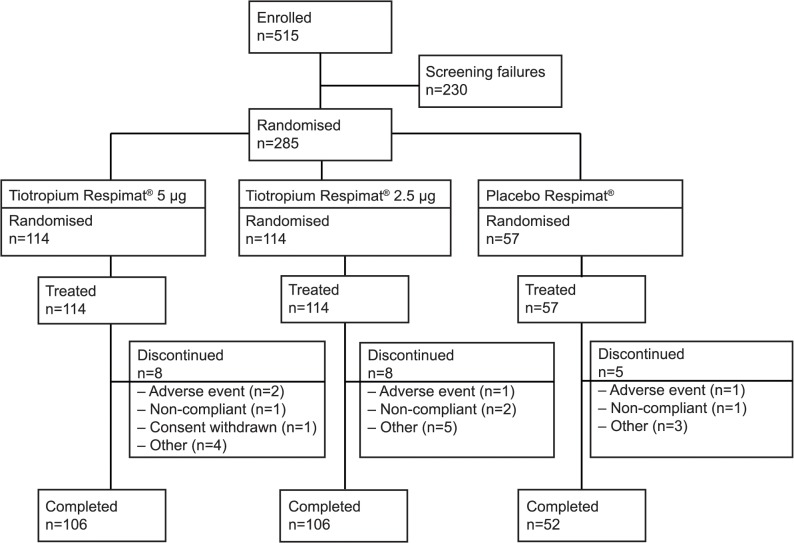
Methods: 285 patients with symptomatic asthma, despite treatment with ICS±LABA, were randomised 2:2:1 to once-daily tiotropium 5 μg, tiotropium 2.5 μg or placebo for 52 weeks (via the Respimat SoftMist inhaler) added on to ICS±LABA, in a double-blind, placebo-controlled, parallel-group study (NCT01340209).
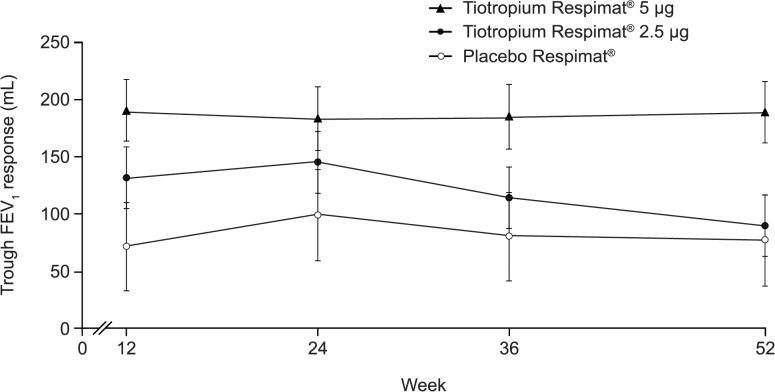
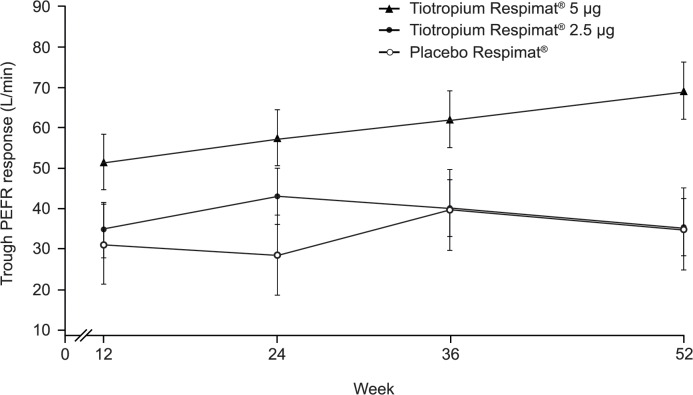
Primary objective: to describe the long-term safety profile of tiotropium. Secondary end points included: trough forced expiratory volume in 1 second (FEV1) response; peak expiratory flow rate (PEFR) response; seven-question Asthma Control Questionnaire (ACQ-7) score.
Results: At Week 52, adverse-event (AE) rates with tiotropium 5 μg, 2.5 μg and placebo were 88.6%, 86.8% and 89.5%, respectively. Commonly reported AEs with tiotropium 5 μg, 2.5 μg and placebo were nasopharyngitis (48.2%, 44.7%, 42.1%), asthma (28.9%, 29.8%, 38.6%), decreased PEFR (15.8%, 7.9%, 21.1%), bronchitis (9.6%, 13.2%, 7.0%), pharyngitis (7.9%, 13.2%, 3.5%) and gastroenteritis (10.5%, 3.5%, 5.3%). In the tiotropium 5 μg, 2.5 μg and placebo groups, 8.8%, 5.3% and 5.3% of patients reported drug-related AEs; 3.5%, 3.5% and 15.8% reported serious AEs. Asthma worsening was the only serious AE reported in more than one patient. At Week 52, adjusted mean trough FEV1 and trough PEFR responses were significantly higher with tiotropium 5 μg (but not 2.5 μg) versus placebo. ACQ-7 responder rates were higher with tiotropium 5 μg and 2.5 μg versus placebo at Week 24.
Conclusions: The long-term tiotropium Respimat safety profile was comparable with that of placebo Respimat, and associated with mild to moderate, non-serious AEs in patients with symptomatic asthma despite ICS±LABA therapy. Compared with placebo, tiotropium 5 μg, but not 2.5 μg, significantly improved lung function and symptoms, supporting the long-term efficacy of the 5 μg dose.
Trial registration: ClinicalTrials.gov NCT01340209.
Conflict of interest statement
Figures
References
-
- Global Initiative for Asthma. Global strategy for asthma management and prevention. Revised 2014. Available: http://www.ginasthma.org/local/uploads/files/GINA_Report_2014_Jun11.pdf. Accessed 12 June 2014.
-
- Masoli M, Fabian D, Holt S, Beasley R, Global Initiative for Asthma (GINA) Program. The global burden of asthma: executive summary of the GINA Dissemination Committee report. Allergy. 2004;59:469–478. - PubMed
-
- Bateman ED, Boushey HA, Bousquet J, Busse WW, Clark TJH, Pauwels RA, et al. Can guideline-defined asthma control be achieved? The Gaining Optimal Asthma ControL study. Am J Respir Crit Care Med. 2004;170:836–844. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
