

Panitumumab in Metastatic Colorectal Cancer: The Importance of Tumour RAS Status
- PMID: 25895463
- PMCID: PMC4419154
- DOI: 10.1007/s40265-015-0386-x
Panitumumab in Metastatic Colorectal Cancer: The Importance of Tumour RAS Status
Abstract
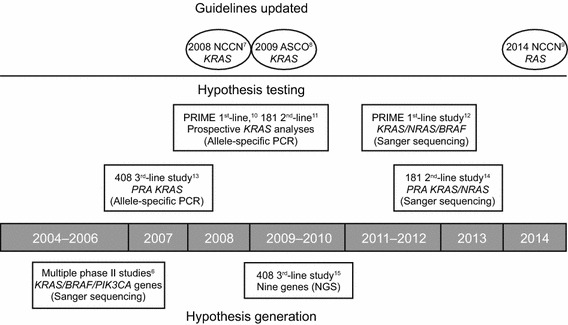
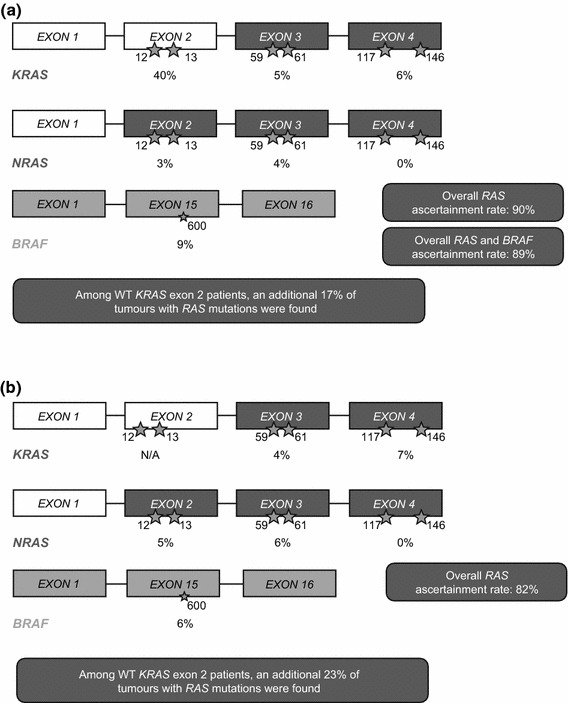
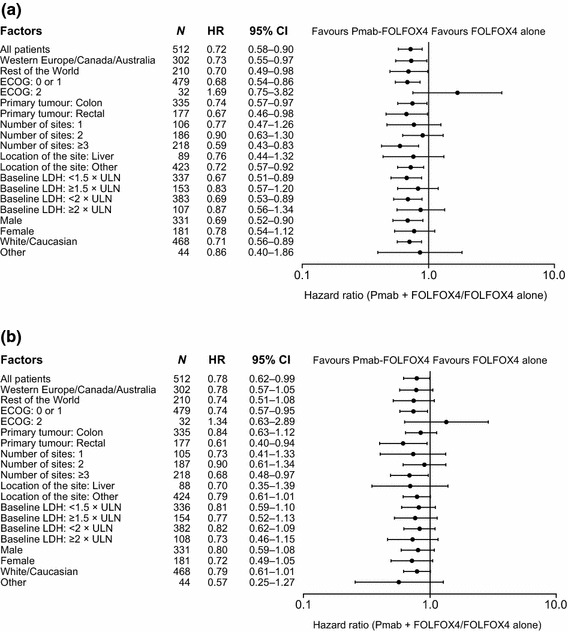
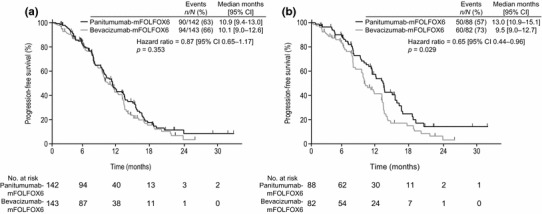
Tumour biomarker status is being used more and more frequently to guide treatment decisions in patients with metastatic colorectal cancer (mCRC). Continued cycles of hypothesis generation and biomarker testing in retrospective, prospective-retrospective and prospective analyses from studies of the epidermal growth factor (EGFR)-targeted monoclonal antibodies (mAbs), panitumumab and cetuximab, have resulted in improved patient selection in mCRC. Initial data suggested EGFR-targeted mAb treatment should be limited to patients with KRAS exon 2 wild-type (WT) tumours, but the availability of tumour samples from large phase III studies permitted evaluation of additional potential biomarkers of activity for these agents. Subsequent analyses further refined the target population to those patients whose tumours were WT for KRAS and NRAS exons 2, 3 and 4 (i.e., those with RAS WT status). Here, we review key clinical data for panitumumab in mCRC across the lines of treatment, assessing in detail the impact of more comprehensive RAS selection on patient outcomes. Panitumumab data across first- to third-line therapy consistently demonstrate that by testing tumour RAS status, it is possible to select patients more likely to benefit from treatment.
Figures
References
-
- Benvenuti S, Sartore-Bianchi A, Di Nicolantonio F, Zanon C, Moroni M, Veronese S, et al. Oncogenic activation of the RAS/RAF signaling pathway impairs the response of metastatic colorectal cancers to anti-epidermal growth factor receptor antibody therapies. Cancer Res. 2007;67(6):2643–2648. doi: 10.1158/0008-5472.CAN-06-4158. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
