

Update on the management of rosacea
- PMID: 25897253
- PMCID: PMC4396587
- DOI: 10.2147/CCID.S58940
Update on the management of rosacea
Abstract
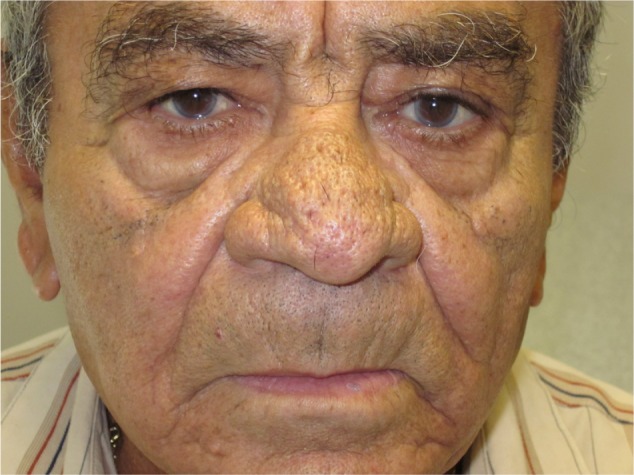
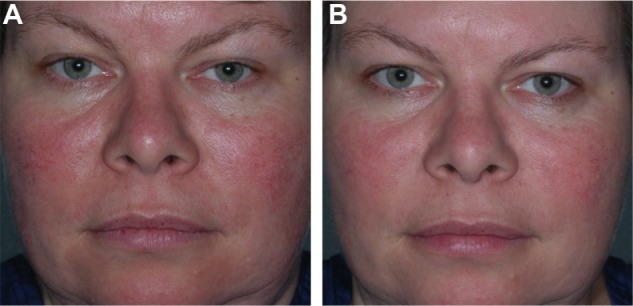
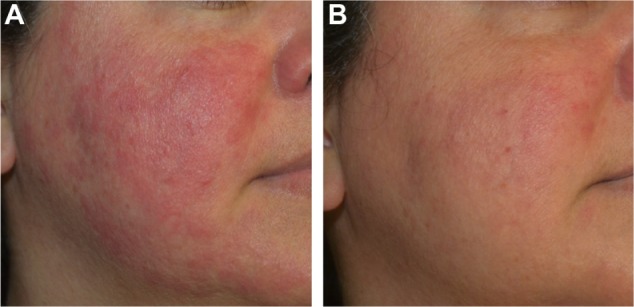
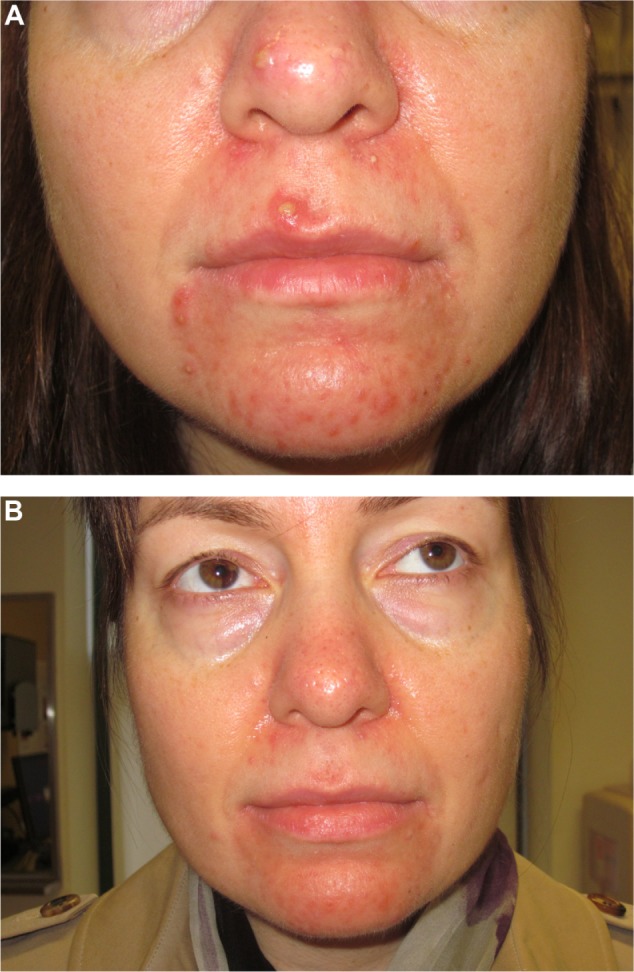
Refining diagnostic criteria has identified key characteristics differentiating rosacea, a chronic skin disorder, from other common cutaneous inflammatory conditions. The current classification system developed by the National Rosacea Society Expert Committee consists of erythematotelangiectatic, papulopustular, phymatous, and ocular subtypes. Each subtype stands as a unique entity among a spectrum, with characteristic symptoms and physical findings, along with an intricate pathophysiology. The main treatment modalities for rosacea include topical, systemic, laser, and light therapies. Topical brimonidine tartrate gel and calcineurin inhibitors are at the forefront of topical therapies, alone or in combination with traditional therapies such as topical metronidazole or azelaic acid and oral tetracyclines or isotretinoin. Vascular laser and intense pulsed light therapies are beneficial for the erythema and telangiectasia, as well as the symptoms (itching, burning, pain, stinging, swelling) of rosacea. Injectable botulinum toxin, topical ivermectin, and microsecond long-pulsed neodymium-yttrium aluminum garnet laser are emerging therapies that may prove to be extremely beneficial in the future. Once a debilitating disorder, rosacea has become a well known and manageable entity in the setting of numerous emerging therapeutic options. Herein, we describe the treatments currently available and give our opinions regarding emerging and combination therapies.
Keywords: guidelines; management; rhinophyma; rosacea; vascular laser.
Figures



Republished in
-
Update on the Management of Rosacea.Plast Surg Nurs. 2015 Oct-Dec;35(4):184-202. doi: 10.1097/PSN.0000000000000111. Plast Surg Nurs. 2015. PMID: 26605825
References
-
- Cribier B. Medical history of the representation of rosacea in the 19th century. J Am Acad Dermatol. 2013;69(6 Suppl 1):S2–S14. - PubMed
-
- Crawford GH, Pelle MT, James WD. Rosacea: I. Etiology pathogenesis, and subtype classification. J Am Acad Dermatol. 2004;51(3):327–341. - PubMed
-
- Wilkin J, Dahl M, Detmar M, et al. Standard classification of rosacea: Report of the National Rosacea Society Expert Committee on the classification and staging of rosacea. J Am Acad Dermatol. 2002;46(4):584–587. - PubMed
-
- Abram K, Silm H, Oona M. Prevalence of rosacea in an Estonian working population using a standard classification. Acta Derm Venereol. 2010;90(3):269–273. - PubMed
-
- Tan J, Berg M. Rosacea: current state of epidemiology. J Am Acad Dermatol. 2013;69(6 Suppl 1):S27–S35. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
