

Occipital condyle fracture and lower cranial nerve palsy after blunt head trauma - a literature review and case report
- PMID: 25897322
- PMCID: PMC4403883
- DOI: 10.1186/s13032-015-0024-3
Occipital condyle fracture and lower cranial nerve palsy after blunt head trauma - a literature review and case report
Abstract
Background: Lower cranial nerve (IX-XII) palsy is a rare condition with numerous causes, usually non-traumatic. In the literature it has been described only a few times after trauma, mostly accompanied by a fracture of the occipital condyle. Although these types of fractures have rarely been reported one could suspect they have been under-diagnosed. During the past decade they have been seen more frequently, most probably due to increased use of CT- and MRI-scanning. The purpose of this review is to increase the awareness of complications following injuries in the craniocervical region.
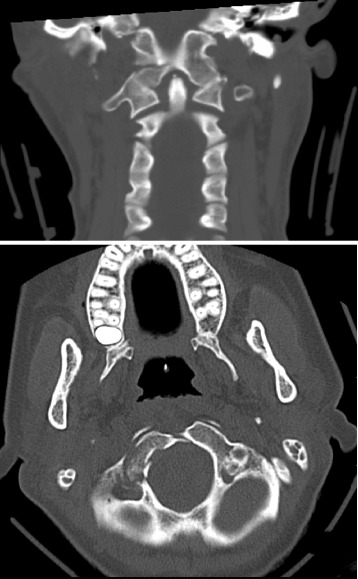
Methods: We based this article on a retrospective review of the medical record of a 24-year old woman admitted to our trauma center after being involved in a car accident and a review of the literature on occipital condyle fractures associated with lower cranial nerve palsy.
Results: The multitraumatized patient had suffered a dislocated occipital condyle fracture. Months later she was diagnosed with palsy to cranial nerve IX-XII. Literature review shows that occipital condyle fractures are rare as isolated injuries and are in many cases accompanied by further injuries to the cervical spine and soft tissue structures, in many cases ending with severe disability. The exact mechanism leading to these injuries cannot always be explained.
Conclusion: Recognition of soft tissue injuries in patients with blunt head trauma is important. CT findings involving the craniocervical junction in these patients advocates further investigations including a thorough neurological examination and liberal use of MRI.
Keywords: Collet-Sicard-Syndrome; Cranial nerve palsy; Occipital condyle fracture.
Figures


References
-
- Collet FJ. Sur un novueau syndrome paralytique pharyngolarynge par blessure de guerre (Hemiplegie glosso-laryngo-scapulo-pharyngee) Lyon Med. 1915;124:121–9.
-
- Sicard J. Syndrome de carrefour condylo-dechire posterieur (type purde paralysie laryngee assiciee) Marseille Med. 1917;53:383.
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
