

Perioperative fluid therapy: a statement from the international Fluid Optimization Group
- PMID: 25897397
- PMCID: PMC4403901
- DOI: 10.1186/s13741-015-0014-z
Perioperative fluid therapy: a statement from the international Fluid Optimization Group
Abstract
Background: Perioperative fluid therapy remains a highly debated topic. Its purpose is to maintain or restore effective circulating blood volume during the immediate perioperative period. Maintaining effective circulating blood volume and pressure are key components of assuring adequate organ perfusion while avoiding the risks associated with either organ hypo- or hyperperfusion. Relative to perioperative fluid therapy, three inescapable conclusions exist: overhydration is bad, underhydration is bad, and what we assume about the fluid status of our patients may be incorrect. There is wide variability of practice, both between individuals and institutions. The aims of this paper are to clearly define the risks and benefits of fluid choices within the perioperative space, to describe current evidence-based methodologies for their administration, and ultimately to reduce the variability with which perioperative fluids are administered.
Methods: Based on the abovementioned acknowledgements, a group of 72 researchers, well known within the field of fluid resuscitation, were invited, via email, to attend a meeting that was held in Chicago in 2011 to discuss perioperative fluid therapy. From the 72 invitees, 14 researchers representing 7 countries attended, and thus, the international Fluid Optimization Group (FOG) came into existence. These researches, working collaboratively, have reviewed the data from 162 different fluid resuscitation papers including both operative and intensive care unit populations. This manuscript is the result of 3 years of evidence-based, discussions, analysis, and synthesis of the currently known risks and benefits of individual fluids and the best methods for administering them.
Results: The results of this review paper provide an overview of the components of an effective perioperative fluid administration plan and address both the physiologic principles and outcomes of fluid administration.
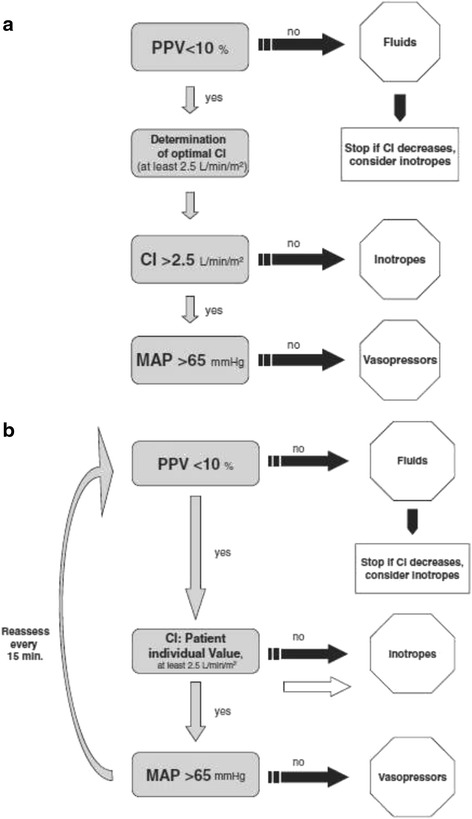
Conclusions: We recommend that both perioperative fluid choice and therapy be individualized. Patients should receive fluid therapy guided by predefined physiologic targets. Specifically, fluids should be administered when patients require augmentation of their perfusion and are also volume responsive. This paper provides a general approach to fluid therapy and practical recommendations.
Keywords: Fluid responsiveness; Fluid resuscitation; Goal-directed fluid therapy; Perioperative fluids.
Figures

References
-
- Dimick JB, Chen SL, Taheri PA, Henderson WG, Khuri SF, Campbell DA., Jr Hospital costs associated with surgical complications: a report from the private-sector National Surgical Quality Improvement Program. J Am Coll Surg. 2004;199:531–7. - PubMed
-
- Bellamy MC. Wet, dry or something else? Br J Anaesth. 2006;97:755–7. - PubMed
-
- Doherty M, Buggy DJ. Intraoperative fluids: how much is too much? Br J Anaesth. 2012;109:69–79. - PubMed
-
- Holte K, Sharrock NE, Kehlet H. Pathophysiology and clinical implications of perioperative fluid excess. Br J Anaesth. 2002;89:622–32. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
