

Red blood cell transfusion for people undergoing hip fracture surgery
- PMID: 25897628
- PMCID: PMC11065123
- DOI: 10.1002/14651858.CD009699.pub2
Red blood cell transfusion for people undergoing hip fracture surgery
Abstract
Background: The incidence of hip fracture is increasing and it is more common with increasing age. Surgery is used for almost all hip fractures. Blood loss occurs as a consequence of both the fracture and the surgery and thus red blood cell transfusion is frequently used. However, red blood cell transfusion is not without risks. Therefore, it is important to identify the evidence for the effective and safe use of red blood cell transfusion in people with hip fracture.
Objectives: To assess the effects (benefits and harms) of red blood cell transfusion in people undergoing surgery for hip fracture.
Search methods: We searched the Cochrane Bone, Joint and Muscle Trauma Group Specialised Register (31 October 2014), the Cochrane Central Register of Controlled Trials (The Cochrane Library, 2014, Issue 10), MEDLINE (January 1946 to 20 November 2014), EMBASE (January 1974 to 20 November 2014), CINAHL (January 1982 to 20 November 2014), British Nursing Index Database (January 1992 to 20 November 2014), the Systematic Review Initiative's Transfusion Evidence Library, PubMed for e-publications, various other databases and ongoing trial registers.
Selection criteria: Randomised controlled trials comparing red blood cell transfusion versus no transfusion or an alternative to transfusion, different transfusion protocols or different transfusion thresholds in people undergoing surgery for hip fracture.
Data collection and analysis: Three review authors independently assessed each study's risk of bias and extracted data using a study-specific form. We pooled data where there was homogeneity in the trial comparisons and the timing of outcome measurement. We used GRADE criteria to assess the quality (low, moderate or high) of the evidence for each outcome.
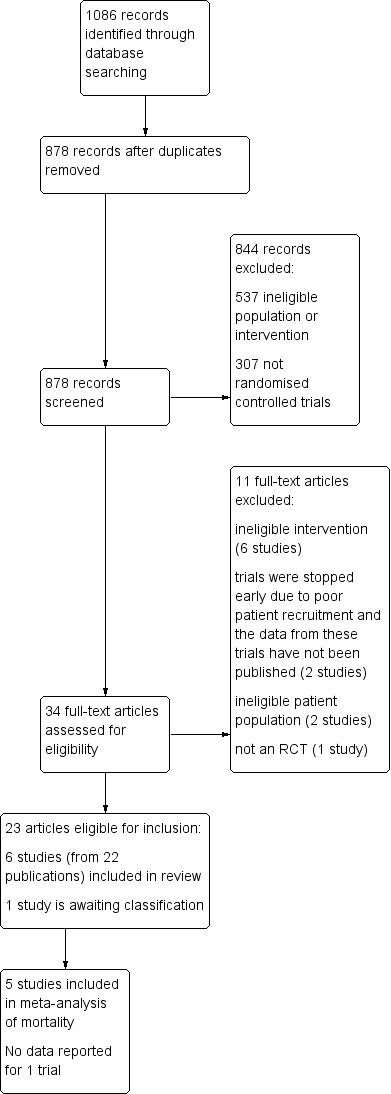
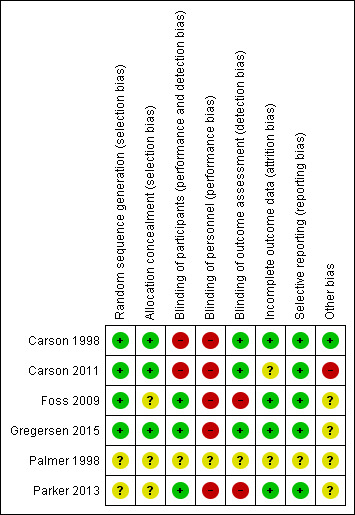
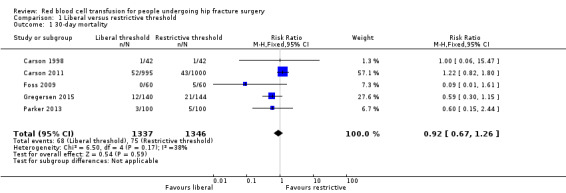
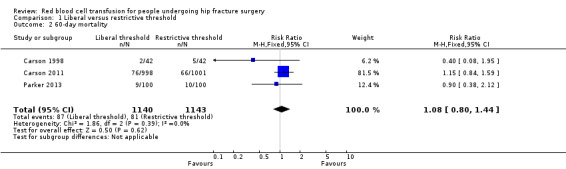
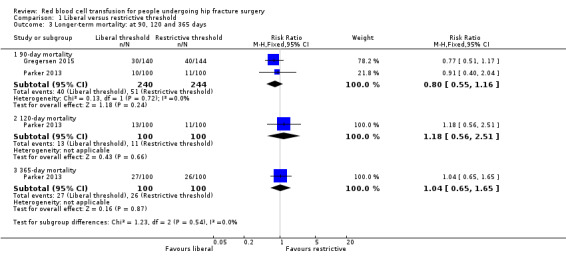
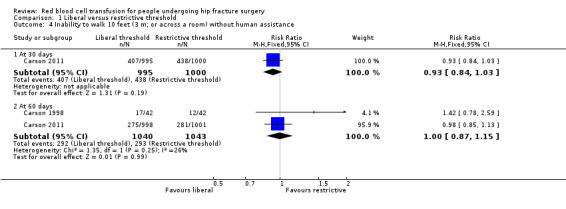
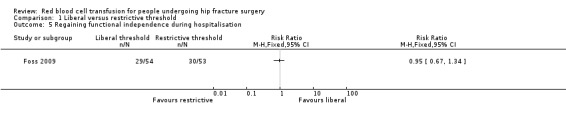
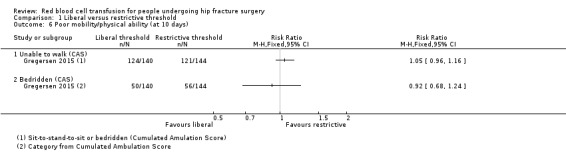
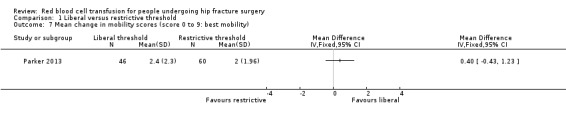
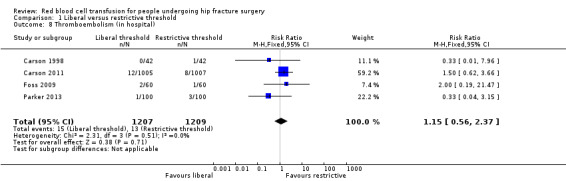
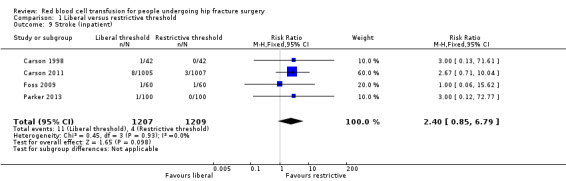
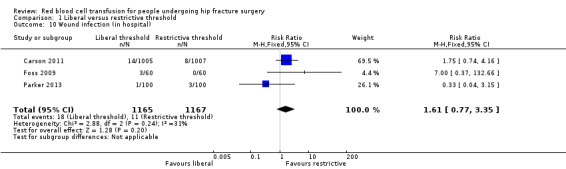
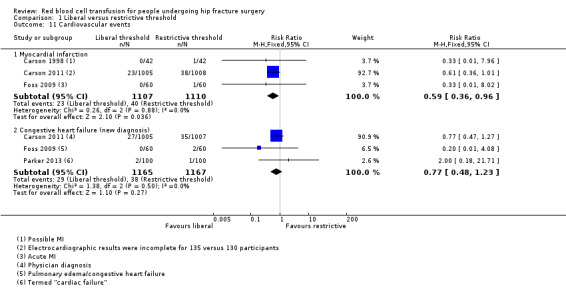
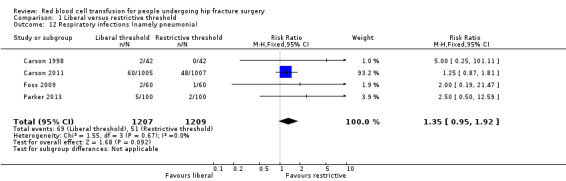
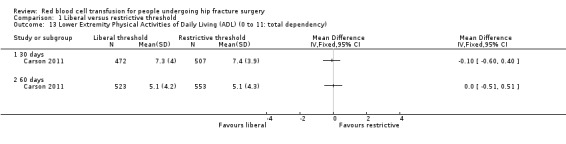
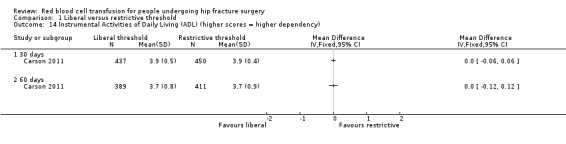
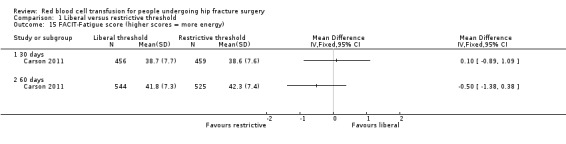
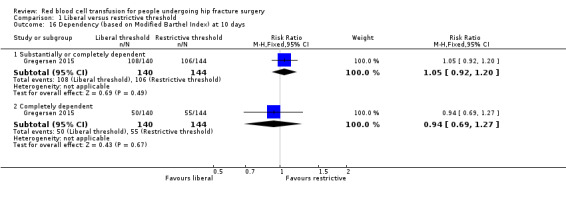
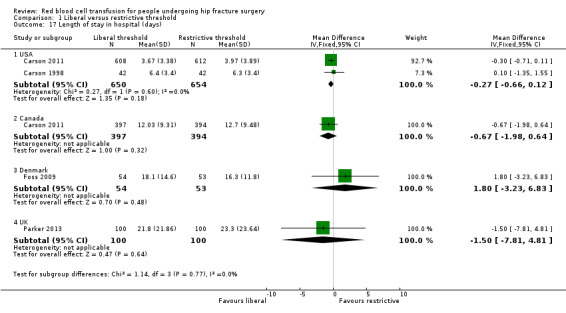
Main results: We included six trials (2722 participants): all compared two thresholds for red blood cell transfusion: a 'liberal' strategy to maintain a haemoglobin concentration of usually 10 g/dL versus a more 'restrictive' strategy based on symptoms of anaemia or a lower haemoglobin concentration, usually 8 g/dL. The exact nature of the transfusion interventions, types of surgery and participants varied between trials. The mean age of participants ranged from 81 to 87 years and approximately 24% of participants were men. The largest trial enrolled 2016 participants, over 60% of whom had a history of cardiovascular disease. The percentage of participants receiving a red blood cell transfusion ranged from 74% to 100% in the liberal transfusion threshold group and from 11% to 45% in the restrictive transfusion threshold group. There were no results available for the smallest trial (18 participants). All studies were at some risk of bias, in particular performance bias relating to the absence of blinding of personnel. We judged the evidence for all outcomes, except myocardial infarction, was low quality reflecting risk of bias primarily from imbalances in protocol violations in the largest trial and imprecision, often because of insufficient events. Thus, further research is likely to have an important impact on these results.There was no evidence of a difference between a liberal versus restricted threshold transfusion in mortality, at 30 days post hip fracture surgery (risk ratio (RR) 0.92, 95% confidence interval (CI) 0.67 to 1.26; five trials; 2683 participants; low quality evidence) or at 60 days post surgery (RR 1.08, 95% CI 0.80 to 1.44; three trials; 2283 participants; low quality evidence). Assuming an illustrative baseline risk of 50 deaths per 1000 participants in the restricted threshold group at 30 days, these data equate to four fewer (95% CI 17 fewer to 14 more) deaths per 1000 in the liberal threshold group at 30 days.There was no evidence of a difference between a liberal versus restricted threshold transfusion in functional recovery at 60 days, assessed in terms of the inability to walk 10 feet (3 m) without human assistance (RR 1.00, 95% CI 0.87 to 1.15; two trials; 2083 participants; low quality evidence).There was low quality evidence of no difference between the transfusion thresholds in postoperative morbidity for the following complications: thromboembolism (RR 1.15 favouring a restrictive threshold, 95% CI 0.56 to 2.37; four trials; 2416 participants), stroke (RR 2.40 favouring a restrictive threshold, 95% CI 0.85 to 6.79; four trials; 2416 participants), wound infection (RR 1.61 favouring a restrictive threshold, 95% CI 0.77 to 3.35; three trials; 2332 participants), respiratory infection (pneumonia) (RR 1.35 favouring a restrictive threshold, 95% CI 0.95 to 1.92; four trials; 2416 participants) and new diagnosis of congestive heart failure (RR 0.77 favouring a liberal threshold, 95% CI 0.48 to 1.23; three trials; 2332 participants). There was very low quality evidence of a lower risk of myocardial infarction in the liberal compared with the restrictive transfusion threshold group (RR 0.59, 95% CI 0.36 to 0.96; three trials; 2217 participants). Assuming an illustrative baseline risk of myocardial infarction of 24 per 1000 participants in the restricted threshold group, this result was compatible with between one and 15 fewer myocardial infarctions in the liberal threshold group.
Authors' conclusions: We found low quality evidence of no difference in mortality, functional recovery or postoperative morbidity between 'liberal' versus 'restrictive' thresholds for red blood cell transfusion in people undergoing surgery for hip fracture. Although further research may change the estimates of effect, the currently available evidence does not support the use of liberal red blood cell transfusion thresholds based on a 10 g/dL haemoglobin trigger in preference to more restrictive transfusion thresholds based on lower haemoglobin levels or symptoms of anaemia in these people. Future research needs to address the effectiveness of red blood cell transfusions at different time points in the surgical pathway, whether pre-operative, peri-operative or postoperative. In particular, such research would need to consider people who are symptomatic or haemodynamically unstable who were excluded from most of these trials.
Conflict of interest statement
Ali Shokoohi: none. Sarah L Millette: none. Susan J Brunskill: none. E Claire Pulford: none. Carolyn Dorée: none. Michael F Murphy: none. Simon Stanworth: none.
Figures
Update of
References
References to studies included in this review
Carson 1998 {published data only}
-
- Brunskill SJ [per comm]. Pilot to the FOCUS trial. Email to: J Carson 7 March 2013.
-
- Carson JL, Terrin ML, Barton FB, Aaron R, Greenburg AG, Heck DA, et al. A pilot randomized trial comparing symptomatic vs. hemoglobin‐level‐driven red blood cell transfusions following hip fracture. Transfusion 1998;28(6):522‐9. - PubMed
Carson 2011 {published data only}
-
- Barr PJ, Bailie KEM. Transfusion thresholds in FOCUS. New England Journal of Medicine 2011;365(26):2532‐3. - PubMed
-
- Brunskill SJ [per comm]. FOCUS trial. Email to: J Carson 7 March 2013.
-
- Carson J. FOCUS: transfusion triggers after fractured hip repair. Transfusion Medicine 2011;21:14.
-
- Carson J. Safety and effectiveness of two blood transfusion strategies in surgical patient with cardiovascular disease (FOCUS). clinicaltrials.gov/show/NCT00071032 (accessed 21 July 2014).
-
- Carson J. Transfusion triggers in orthopedic patients. Transfusion Alternatives in Transfusion Medicine 2011;12(1):9.
Foss 2009 {published data only}
-
- Brunskill SJ [pers comms]. Cochrane review transfusion in hip fracture ‐ request for information. Email to N Foss 4 September 2014.
-
- Foss N. The effect of liberal vs. restrictive transfusion strategies on rehabilitation after hip fracture surgery. clinicaltrials.gov/show/NCT00162617 (accessed 21 July 2014).
-
- Foss NB, Kristensen MT, Jensen PS, Palm H, Krasheninnikoff M, Kehlet H. The effects of liberal versus restrictive transfusion thresholds on ambulation after hip fracture surgery. Transfusion 2009;49(2):227‐34. - PubMed
-
- Pulford EC [pers comms]. Cochrane review transfusion in hip fracture ‐ request for information. Email to: Nocolai Foss 3 May 2013.
Gregersen 2015 {published data only}
-
- Brunskill SJ [pers comms]. Cochrane review transfusion in hip fracture ‐ request for information. Email to M Gregersen 11 December 2014.
-
- Gregersen M. Postoperative blood transfusion for frail elderly with hip fracture. clinicaltrials.gov/show/NCT01102010 (accessed 21 July 2014).
-
- Gregersen M, Borris LC, Damsgaard EM. A liberal blood transfusion strategy after hip fracture surgery does not increase the risk of infection in frail elderly. European Geriatric Medicine 2012;3 Suppl:S74.
-
- Gregersen M, Borris LC, Damsgaard EM. A liberal blood transfusion strategy improves survival in nursing home residents with hip fracture. European Geriatric Medicine 2013;4 Suppl:S106.
-
- Gregersen M, Borris LC, Damsgarrd EM. Postoperative blood transfusion strategy in frail anemic elderly with hip fracture: the TRIFE randomised controlled trial. Acta Orthopaedica 2015 (Posted online on January 14, 2015);86(3):1‐10 (online version numbering). [DOI: 10.3109/17453674.2015.1006980] - DOI - PMC - PubMed
Palmer 1998 {published data only}
-
- Brunskill SJ [pers comm]. Conference abstract ‐ British Blood Transfusion Society meeting 1998 ‐ Hip fracture and transfusion trial (HATT). Email to: B McClelland 24 January 2013.
-
- Palmer JB, Maciver CR, Scott R, Picken MG, McClelland DBL, Keating JF, et al. Hip fracture and transfusion trial (HATT). Transfusion Medicine 1998;8 Suppl:Abstract P52.
Parker 2013 {published data only}
-
- Brunskill SJ [pers comm]. Randomised trial of a blood transfusion policy after fracture of the proximal femur (hip fracture). Email to: M Parker 14 March 2013.
-
- Parker M. Randomised trial of a blood transfusion policy after fracture of the proximal femur (hip fracture). www.controlled‐trials.com/ISRCTN61328173 (accessed 21 July 2014).
-
- Parker M. Randomised trial of blood transfusion versus a restrictive transfusion policy after hip fracture surgery. Injury 2013;44(12):1916‐8. - PubMed
References to studies excluded from this review
Gampopoulou 2004 {published data only}
-
- Gampopoulou Z, Vretou V, Mauromati P, Chatzieleftheriou A, Vasilaki M, Papadimos M, et al. Red cell transfusion with and without leukocyte depletion for orthopedic surgery. Transfusion Alternatives in Transfusion Medicine 2004;6 Suppl:P20.
Izuel‐Rami 2005 {published data only}
-
- Izuel‐Rami M, Cuenca Espirrez J, Garcia‐Erce JA, Gomez‐Barrera M, Carceln Andreas J, Rabanaque Herníndez MJ. Perioperative anaemia in geriatric patients with hip fracture [Efectividad de distintas pautas de tratamiento de la anemia perioperatoria en pacientes ancianos con fractura de cadera]. Farmacia Hospitalaria 2005;29(4):250‐7. - PubMed
Izuel‐Rami 2006 {published data only}
-
- Izuel‐Rami M, Garcia‐Erce JA, Cuenca J, Gomez‐Barrera M, Villar I, Rabanaque MJ. Recovery from postoperative anaemia after hip fracture replacement surgery. Is there a role for erythropoietin and intravenous iron?. Transfusion Alternatives in Transfusion Medicine 2006;8 Suppl:P53.
Jans 2011 {published data only}
-
- Jans O. Liberal versus restrictive transfusion during symptomatic moderate anemia after hip arthroplasty. clinicaltrials.gov/show/NCT01452581 (accessed 21 July 2014).
Matot 2012 {published data only}
-
- Brunskill SJ [pers comm]. NCT01491308, TASMAC‐11‐IM‐0449‐11‐CTIL, Restrictive versus liberal red cell transfusion strategy in orthopedic‐oncology patients undergoing surgery ‐ a randomized controlled study. Email to: Idit Matot 14 March 2013.
-
- Matot I. Restrictive versus liberal red cell transfusion strategy in orthopedic‐oncology patients undergoing surgery ‐ a randomized controlled study. clinicaltrials.gov/show/NCT01491308 (accessed 21 July 2014).
Moghaddam 2009 {published data only}
-
- Moghaddam MJ, Razavi SS, Momenzadeh S, Radfar A. The effects of tranexamic acid on hemorrhage in femoral fracture surgery. Journal of the Faculty of Medicine 2009;33(2):3.
Muir 1995 {published data only}
Nielsen 2012 {published data only}
-
- Brunskill SJ [pers comm]. Establishment of optimal transfusion threshold after major orthopedic surgery. Email to: K Neilsen 14 March 2013.
-
- Nielsen K. Establishment of optimal transfusion threshold after major orthopedic surgery. clinicaltrials.gov/ct2/show/NCT00906295 (accessed 21 July 2014).
Prasad 2009 {published data only}
-
- Prasad N, Rajamani V, Hullin D, Murray JM. Post‐operative anaemia in femoral neck fracture patients: does it need treatment? A single blinded prospective randomised controlled trial. Injury 2009;40(10):1073‐6. - PubMed
Serrano Trenas 2011 {published data only}
-
- Serrano‐Trenas JA, Ugalde PF, Cabello LM, Chofles LC, Lázaro PS, Benítez PC. Role of perioperative intravenous iron therapy in elderly hip fracture patients: a single‐center randomized controlled trial. Transfusion 2011;51(1):97‐104. - PubMed
Zufferey 2010 {published data only}
-
- Zufferey PJ, Miquet M, Quenet S, Martin P, Adam P, Albaladejo P, et al. Tranexamic acid in hip fracture surgery: a randomized controlled trial. British Journal of Anaesthesia 2010;104(1):23‐30. - PubMed
References to studies awaiting assessment
ChiCTR‐TRC‐10000822 {published data only}
-
- Wu Q. Clinical research of restrictive transfusion in elderly patients undergoing orthopedic surgery. apps.who.int/trialsearch/Trial.aspx?TrialID=ChiCTR‐TRC‐10000822 (accessed 21 July 2014).
Additional references
Adunsky 2008
-
- Adunsky A, Arad M, Blumstein T, Weitzman A, Mizrahi EH. Discharge hemoglobin and functional outcome of elderly hip fractured patients undergoing rehabilitation. European Journal of Physical and Rehabilitation Medicine 2008;44(4):417‐22. - PubMed
Carless 2010
Carson 1999
-
- Carson JL, Altman DG, Duff A, Noveck H, Weinstein MP, Sonnenberg FA, et al. Risk of bacterial infection associated with allogeneic blood transfusion among patients undergoing hip fracture repair. Transfusion 1999;39(7):694‐700. - PubMed
Carson 2012
Carson 2013
Department of Health Payment by Results team 2012
-
- Department of Health Payment by Results team. A simple guide to Payment by Results. www.gov.uk/government/publications/simple‐guide‐to‐payment‐by‐results (accessed 21 July 2014).
Dillon 2005
-
- Dillon MF, Collins D, Rice J, Murphy PG, Nicholson P, Mac Elwaine J. Preoperative characteristics identify patients with hip fractures at risk of transfusion. Clinical Orthopaedics and Related Research 2005;439:201‐6. - PubMed
Egol 2009
-
- Egol KA, Strauss EJ. Perioperative considerations in geriatric patients with hip fracture: what is the evidence?. Journal of Orthopaedic Trauma 2009;23(6):386‐94. - PubMed
Foss 2006
-
- Foss NB, Kehlet H. Hidden blood loss after surgery for hip fracture. Journal of Bone & Joint Surgery ‐ British Volume 2006;88(8):1053‐9. - PubMed
Foss 2008
-
- Foss NB, Kristensen MT, Kehlet H. Anaemia impedes functional mobility after hip fracture surgery. Age and Aging 2008;37(2):173‐8. - PubMed
Goodnough 2014
-
- Goodnough LT, Murphy MF. Do liberal blood transfusions cause more harm than good?. BMJ 2014;349:g6897. - PubMed
GRADE 2011
-
- Schünemann HJ, Oxman AD, Vist GE, Higgins JPT, Deeks JJ, Glasziou P, et al. Chapter 12: Interpreting results and drawing conclusions. In: Higgins JPT, Green S (editors), Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Gruber‐Baldini 2013
Gullberg 1997
-
- Gullberg B, Johnell O, Kanis JA. World‐wide projections for hip fracture. Osteoporosis International 1997;7:407‐13. - PubMed
Hajjar 2010
-
- Hajjar LA, Vincent JL, Galas FR, Nakamura RE, Silva CM, Santos MH, et al. Transfusion requirements after cardiac surgery: the TRACS randomized controlled trial. JAMA 2010;304(14):1559‐67. - PubMed
Higgins 2011a
-
- Higgins JPT, Altman DG, Sterne JAC. Chapter 8: Assessing risk of bias in included studies. In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Higgins 2011b
-
- Higgins JPT, Deeks JJ, Altman DG. Chapter 16: Special topics in statistics. In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Higgins 2011c
-
- Higgins JPT, Deeks JJ. Chapter 7: Selecting studies and collecting data. In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Hutton 2005
-
- Hutton B, Fergusson D, Tinmouth A, McIntyre L, Kmetic A, Hebert PC. Transfusion rates vary significantly amongst Canadian medical centres. Canadian Journal of Anaesthesia 2005;52(6):581‐90. - PubMed
Johnston 2006
-
- Johnston P, Wynn‐Jones H, Chakravarty D, Boyle A, Parker MJ. Is perioperative blood transfusion a risk factor for mortality or infection after hip fracture?. Journal of Orthopaedic Trauma 2006;20(10):675‐9. - PubMed
Lawrence 2003
-
- Lawrence VA, Silverstein JH, Cornell JE, Pederson T, Noveck H, Carson JL. Higher Hb level is associated with better early functional recovery after hip fracture repair. Transfusion 2003;43(12):1717‐22. - PubMed
Lefebvre 2011
-
- Lefebvre C, Manheimer E, Glanville J. Chapter 6.4.11: Search filters. In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
McClelland 2009
-
- McClelland B, Walsh T. Good blood management: the effective and safe use of blood components. In: Murphy MF, Pamphilon DH editor(s). Practical Transfusion Medicine. 3rd Edition. Oxford: Wiley‐Blackwell, 2009:265‐84.
Penninx 2006
-
- Penninx BW, Pahor M, Woodman RC, Guralnik JM. Anemia in old age is associated with increased mortality and hospitalization. Journals of Gerontology Series A‐Biological Sciences & Medical Sciences 2006;61(5):474‐9. - PubMed
Perel 2013
RevMan 2011 [Computer program]
-
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.1. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2011.
Rohde 2014
Schünemann 2011
-
- Schünemann HJ, Oxman AD, Vist GE, Higgins JPT, Deeks JJ, Glasziou P, et al. Chapter 12: Interpreting results and drawing conclusions. Higgins JPT, Green S (editors), Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Shokoohi 2012a
-
- Shokoohi A, Stanworth S, Mistry D, Lamb S, Staves J, Murphy MF. The risks of red cell transfusion for hip fracture surgery in the elderly. Vox Sanguinis 2012;103(3):223‐30. - PubMed
SHOT 2010
-
- Taylor C (Ed), Cohen H, Mold D, Jones H, et al on behalf of the Serious Hazards of Transfusion (SHOT) Steering Group. The 2009 annual SHOT report. www.shotuk.org/shot‐reports/report‐and‐summary‐2009/ (accessed 21 July 2014).
Smith 2011
-
- Smith GH, Tsang J, Molyneux SG, White TO. The hidden blood loss after hip fracture. Injury 2011;42(2):133‐5. - PubMed
So‐Osman 2013
-
- So‐Osman C, Nelissen R, Brand R, Faber F, Slaa RT, Stiggelbout A, et al. The impact of a restrictive transfusion trigger on post‐operative complication rate and well‐being following elective orthopaedic surgery: a post‐hoc analysis of a randomised study. Blood Transfusion 2013;11(2):289‐95. - PMC - PubMed
Villanueva 2013
-
- Villanueva C, Colomo A, Bosch A, Concepcion M, Hernandez‐Gea V, Aracil C, et al. Transfusion strategies for acute upper gastrointestinal bleeding. New England Journal of Medicine 2013;268(1):11‐21. - PubMed
Walsh 2013
-
- Walsh TS, Boyd JA, Watson D, Hope D, Lewis S, Krishman A, et al. RELIEVE Investigators. Restrictive versus liberal transfusion strategies for older mechanically ventilated critically ill patients: a randomized pilot trial. Critical Care Medicine 2013;41(10):2354‐63. - PubMed
References to other published versions of this review
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical