

Is Urinary Lipoarabinomannan the Result of Renal Tuberculosis? Assessment of the Renal Histology in an Autopsy Cohort of Ugandan HIV-Infected Adults
- PMID: 25897661
- PMCID: PMC4405591
- DOI: 10.1371/journal.pone.0123323
Is Urinary Lipoarabinomannan the Result of Renal Tuberculosis? Assessment of the Renal Histology in an Autopsy Cohort of Ugandan HIV-Infected Adults
Abstract
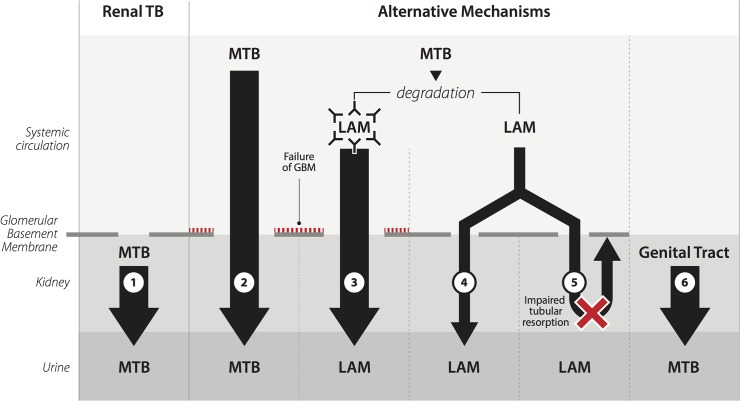
Objective: The detection of urinary lipoarabinomannan (LAM), a mycobacterial cell wall component, is used to diagnose tuberculosis (TB). How LAM enters the urine is not known. To investigate if urinary LAM-positivity is the result of renal TB infection we correlated the outcomes of urinary LAM-antigen testing to renal histology in an autopsy cohort of hospitalized, Ugandan, HIV-infected adults.
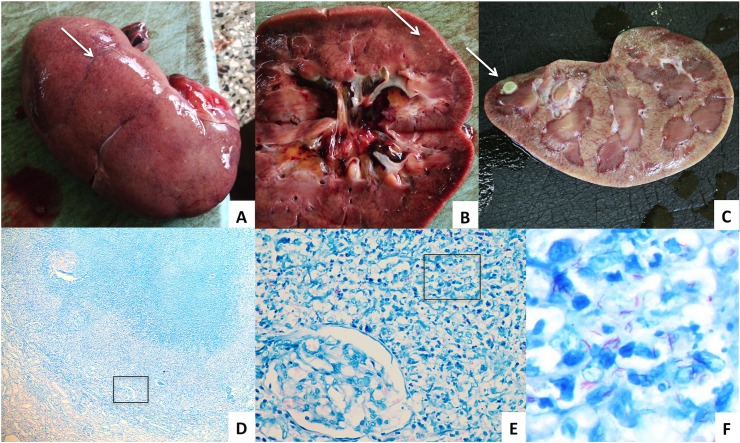
Methods: We performed a complete autopsy, including renal sampling, in HIV-infected adults that died during hospitalization after written informed consent was obtained from the next of kin. Urine was collected postmortem through post-mortem catheterisation or by bladder puncture and tested for LAM with both a lateral flow assay (LFA) and an ELISA assay. Two pathologists assessed the kidney histology. We correlated the LAM-assay results and the histology findings.
Results: Of the 13/36 (36%) patients with a positive urinary LAM ELISA and/or LFA, 8/13 (62%) had renal TB. The remaining 5 LAM-positive patients had disseminated TB without renal involvement. Of the 23 LAM-negative patients, 3 had disseminated TB without renal involvement. The remaining LAM-negative patients had no TB infection and died mostly of fungal and bacterial infections. LAM LFA had a sensitivity of 81% and specificity of 100% to diagnose TB at any location, and the LAM ELISA a sensitivity of 63% and a specificity of 100%. 54% (7/13) LAM LFA-positive patients were not on anti-TB treatment at the time of death.
Conclusion: Renal TB infection explained LAM-positivity in the majority of patients. Patients with disseminated TB without renal involvement can also be diagnosed with LAM. This suggests that other mechanisms that lead to urinary LAM-positivity exist in a minority of patients.
Conflict of interest statement
Figures
References
-
- UNAIDS. AIDS by the numbers. 2013. Available: http://www.unaids.org/sites/default/files/media_asset/JC2571_AIDS_by_the...
-
- World Health Organisation. Global tuberculosis report 2013. 2013. Available: http://apps.who.int/iris/bitstream/10665/91355/1/9789241564656_eng.pdf
-
- World Health Organisation. Estimates of TB and MDR-TB burden. Uganda Tuberculosis Profile. 2015. Available: https://extranet.who.int/sree/Reports?op=Replet&name=/WHO_HQ_Reports/G2/...
-
- Gupta RK, Lawn SD, Bekker LG, Caldwell J, Kaplan R, Wood R. Impact of human immunodeficiency virus and CD4 count on tuberculosis diagnosis: analysis of city-wide data from Cape Town, South Africa. Int J Tuberc Lung Dis. 2013;17(8):1014–22. Epub 2013/07/06. 10.5588/ijtld.13.0032 . - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
