

Impairment of exogenous lactate clearance in experimental hyperdynamic septic shock is not related to total liver hypoperfusion
- PMID: 25898244
- PMCID: PMC4432956
- DOI: 10.1186/s13054-015-0928-3
Impairment of exogenous lactate clearance in experimental hyperdynamic septic shock is not related to total liver hypoperfusion
Abstract
Introduction: Although the prognostic value of persistent hyperlactatemia in septic shock is unequivocal, its physiological determinants are controversial. Particularly, the role of impaired hepatic clearance has been underestimated and is only considered relevant in patients with liver ischemia or cirrhosis. Our objectives were to establish whether endotoxemia impairs whole body net lactate clearance, and to explore a potential role for total liver hypoperfusion during the early phase of septic shock.
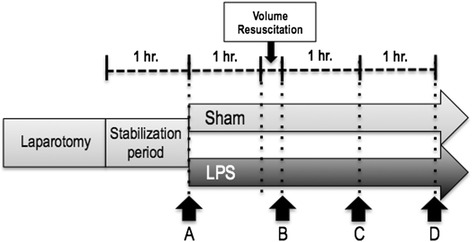
Methods: After anesthesia, 12 sheep were subjected to hemodynamic/perfusion monitoring including hepatic and portal catheterization, and a hepatic ultrasound flow probe. After stabilization (point A), sheep were alternatively assigned to lipopolysaccharide (LPS) (5 mcg/kg bolus followed by 4 mcg/kg/h) or sham for a three-hour study period. After 60 minutes of shock, animals were fluid resuscitated to normalize mean arterial pressure. Repeated series of measurements were performed immediately after fluid resuscitation (point B), and one (point C) and two hours later (point D). Monitoring included systemic and regional hemodynamics, blood gases and lactate measurements, and ex-vivo hepatic mitochondrial respiration at point D. Parallel exogenous lactate and sorbitol clearances were performed at points B and D. Both groups included an intravenous bolus followed by serial blood sampling to draw a curve using the least squares method.
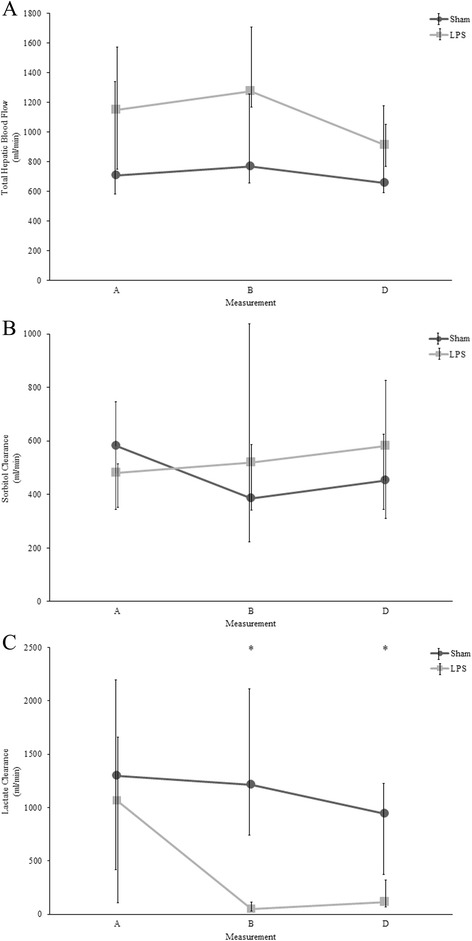
Results: Significant hyperlactatemia was already present in LPS as compared to sham animals at point B (4.7 (3.1 to 6.7) versus 1.8 (1.5 to 3.7) mmol/L), increasing to 10.2 (7.8 to 12.3) mmol/L at point D. A significant increase in portal and hepatic lactate levels in LPS animals was also observed. No within-group difference in hepatic DO2, VO2 or O2 extraction, total hepatic blood flow (point D: 915 (773 to 1,046) versus 655 (593 to 1,175) ml/min), mitochondrial respiration, liver enzymes or sorbitol clearance was found. However, there was a highly significant decrease in lactate clearance in LPS animals (point B: 46 (30 to 180) versus 1,212 (743 to 2,116) ml/min, P < 0.01; point D: 113 (65 to 322) versus 944 (363 to 1,235) ml/min, P < 0.01).
Conclusions: Endotoxemia induces an early and severe impairment in lactate clearance that is not related to total liver hypoperfusion.
Figures
Comment in
-
Is lactate clearance impaired in septic shock?Crit Care. 2015 Sep 10;19(1):306. doi: 10.1186/s13054-015-1039-x. Crit Care. 2015. PMID: 26353812 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
