

Obesity is independently associated with spinal anesthesia outcomes: a prospective observational study
- PMID: 25898360
- PMCID: PMC4405588
- DOI: 10.1371/journal.pone.0124264
Obesity is independently associated with spinal anesthesia outcomes: a prospective observational study
Abstract
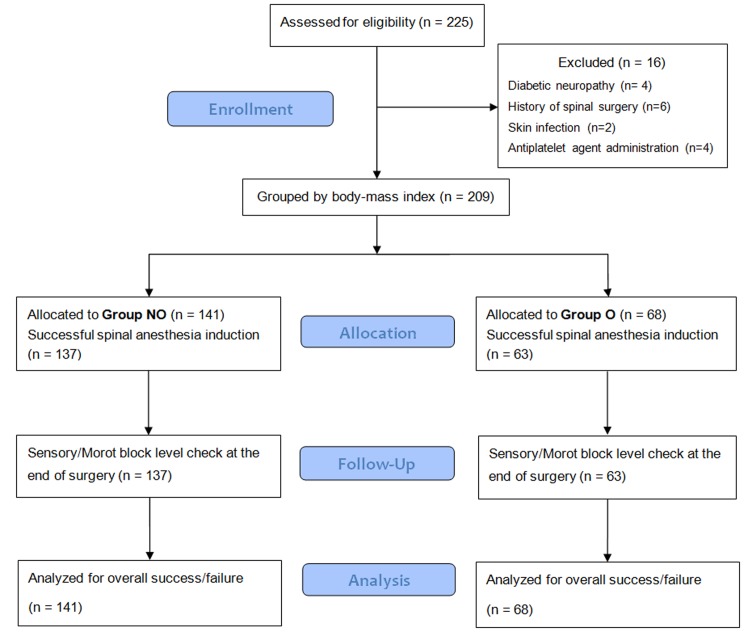
The influence of body-mass index (BMI) on spinal anesthesia is still controversial, with discrepant results reported in previous studies. To compare spinal anesthesia in obese and non-obese subjects, the anesthesia profiles in patients who underwent spinal anesthesia using intrathecal hyperbaric bupivacaine were compared. A total of 209 patients undergoing elective total knee replacement arthroplasty (TKRA) surgery under spinal anesthesia were divided into an NO (non-obese) group (BMI < 30 kg/m2, n = 141) and an O (obese) group (BMI ≥ 30 kg/m2, n = 68). Anesthesia was deemed successful if a bilateral T12 sensory block occurred within 15 minutes of intrathecal drug administration, and if the level of sensory block was higher than T12 when the surgery ended. Logistic regression analysis with multiple variables known to influence spinal anesthesia was performed to identify which parameters independently determined the spinal anesthesia outcome. Similar doses of bupivacaine were administered to the NO and O groups. The incidence of anesthesia failure was significantly lower in the O group [n = 43 (30.5%) in the NO group vs. n = 10 (18.9%) in the O group, p = 0.014]. The independent predictors for successful anesthesia in all patients were dose of hyperbaric bupivacaine [odds ratio (OR) 2.12, 95% CI: 1.64-2.73] and obese status (BMI ≥ 30 kg/m2, OR 2.86, 95% CI: 1.25-6.52). Time to first report of postoperative pain and time to first self-void were significantly longer in the O group. These results suggest that the duration of block with hyperbaric bupivacaine is prolonged in obese patients and obesity is independently associated with spinal anesthesia outcomes, as is bupivacaine dosage. A further study enrolling patients with morbid obesity and using a fixed bupivacaine dosage is required to confirm the effect of obesity on spinal anesthesia.
Conflict of interest statement
Figures

Similar articles
-
The effect of body mass index on spinal anaesthesia for total knee replacement arthroplasty: a dose-response study.Anaesth Intensive Care. 2012 May;40(3):410-6. doi: 10.1177/0310057X1204000305. Anaesth Intensive Care. 2012. PMID: 22577905 Clinical Trial.
-
Does the baricity of bupivacaine influence intrathecal spread in the prolonged sitting position before elective cesarean delivery? A prospective randomized controlled study.Anesth Analg. 2011 Oct;113(4):811-7. doi: 10.1213/ANE.0b013e3182288bf2. Epub 2011 Sep 2. Anesth Analg. 2011. PMID: 21890887 Clinical Trial.
-
ED(50) and ED(95) of intrathecal bupivacaine in morbidly obese patients undergoing cesarean delivery.Anesthesiology. 2011 Mar;114(3):529-35. doi: 10.1097/ALN.0b013e318209a92d. Anesthesiology. 2011. PMID: 21307769 Clinical Trial.
-
ED 50 and ED 95 of intrathecal bupivacaine coadministered with sufentanil for cesarean delivery under combined spinal-epidural in severely preeclamptic patients.Chin Med J (Engl). 2015 Feb 5;128(3):285-90. doi: 10.4103/0366-6999.150083. Chin Med J (Engl). 2015. PMID: 25635420 Free PMC article. Clinical Trial.
-
Childhood obesity: a challenge for the anaesthetist?Paediatr Anaesth. 2002 Nov;12(9):750-61. doi: 10.1046/j.1460-9592.2002.00781.x. Paediatr Anaesth. 2002. PMID: 12519133 Review.
Cited by
-
Type, management, and associated factors of failed spinal anesthesia in cesarean section. Prospective cohort study.Ann Med Surg (Lond). 2022 Apr 22;77:103616. doi: 10.1016/j.amsu.2022.103616. eCollection 2022 May. Ann Med Surg (Lond). 2022. PMID: 35638059 Free PMC article.
-
Incidence and factors associated with failed spinal anaesthesia among patients undergoing surgery: a multi- center prospective observational study.BMC Anesthesiol. 2024 Apr 5;24(1):129. doi: 10.1186/s12871-024-02484-y. BMC Anesthesiol. 2024. PMID: 38580926 Free PMC article.
-
Failed Spinal Anesthesia: Incidence and Associated Factors.Cureus. 2024 Dec 20;16(12):e76078. doi: 10.7759/cureus.76078. eCollection 2024 Dec. Cureus. 2024. PMID: 39835057 Free PMC article.
-
The impact of height on the spread of spinal anesthesia and stress response in parturients undergoing caesarean section: a prospective observational study.BMC Anesthesiol. 2021 Nov 30;21(1):298. doi: 10.1186/s12871-021-01523-2. BMC Anesthesiol. 2021. PMID: 34847868 Free PMC article.
-
Effective Dose Range of Intrathecal Isobaric Bupivacaine to Achieve T5-T10 Sensory Block Heights for Elderly and Overweight Patients: An Observational Study.Medicina (Kaunas). 2023 Mar 1;59(3):484. doi: 10.3390/medicina59030484. Medicina (Kaunas). 2023. PMID: 36984485 Free PMC article.
References
-
- Logan MR, McClure JH, Wildsmith JA. Plain bupivacaine: an unpredictable spinal anaesthetic agent. Br J Anaesth. 1986;58: 292–296. - PubMed
-
- Pitkanen M, Haapaniemi L, Tuominen M, Rosenberg PH. Influence of age on spinal anaesthesia with isobaric 0.5% bupivacaine. Br J Anaesth. 1984;56: 279–284. - PubMed
-
- Pitkanen MT. Body mass and spread of spinal anesthesia with bupivacaine. Anesth Analg. 1987;66: 127–131. - PubMed
-
- Schnider TW, Minto CF, Bruckert H, Mandema JW. Population pharmacodynamic modeling and covariate detection for central neural blockade. Anesthesiology. 1996;85: 502–512. - PubMed
-
- McCulloch WJ, Littlewood DG. Influence of obesity on spinal analgesia with isobaric 0.5% bupivacaine. Br J Anaesth. 1986;58: 610–614. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
