

Utilizing functional lumen imaging probe topography to evaluate esophageal contractility during volumetric distention: a pilot study
- PMID: 25898916
- PMCID: PMC4478241
- DOI: 10.1111/nmo.12572
Utilizing functional lumen imaging probe topography to evaluate esophageal contractility during volumetric distention: a pilot study
Abstract
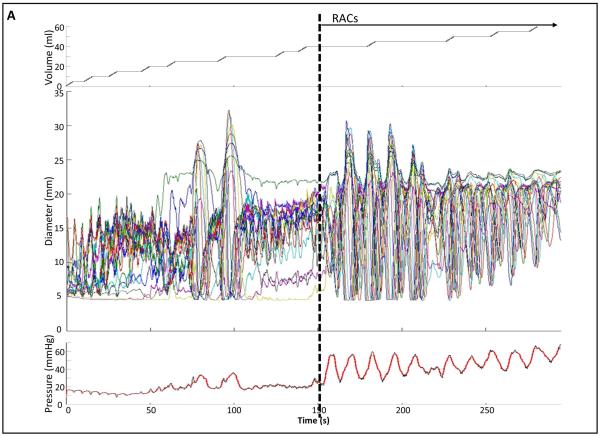
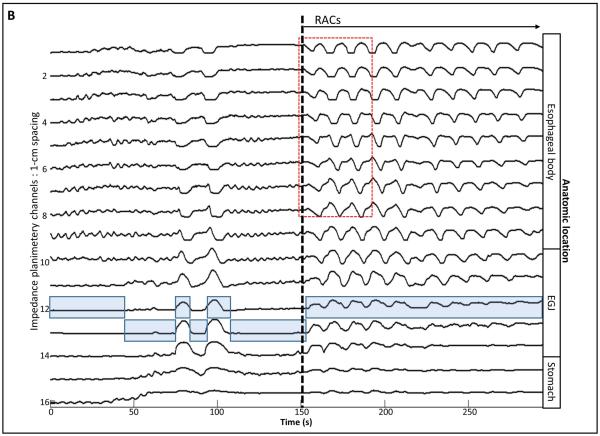
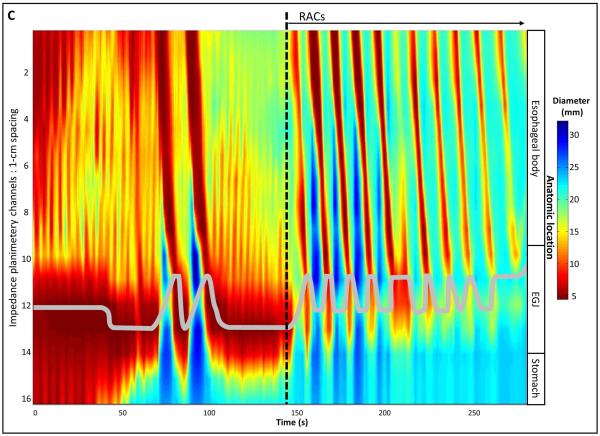
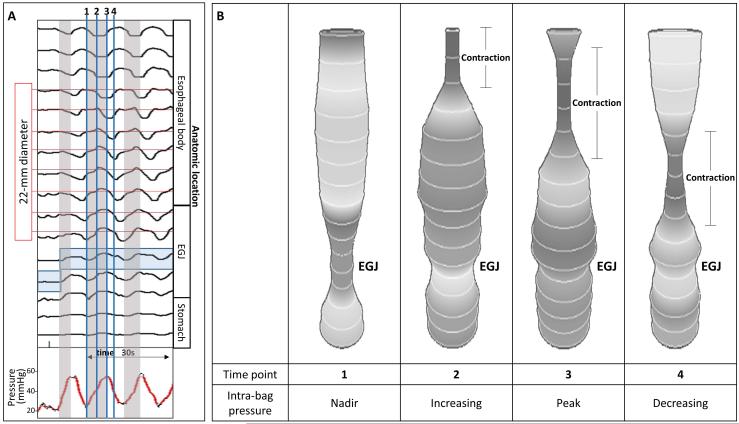
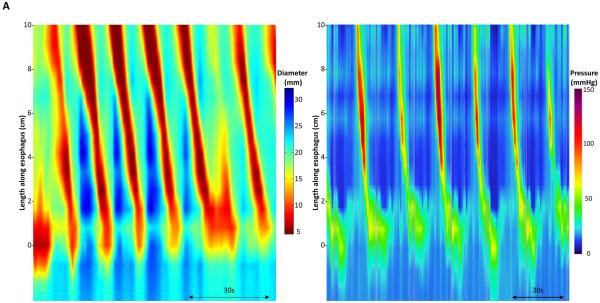
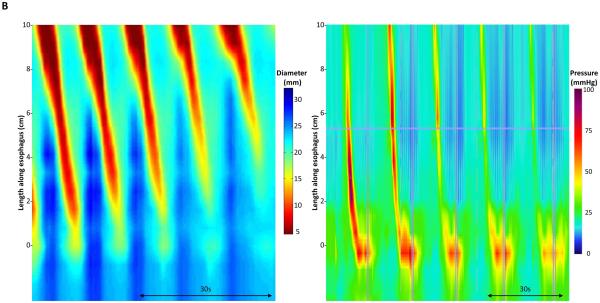
Background: The functional lumen imaging probe (FLIP) measures luminal cross-sectional area and pressure during volumetric distension. By applying novel customized software to produce FLIP topography plots, organized esophageal contractility can be visualized and analyzed. We aimed to describe the stimulus thresholds and contractile characteristics for distension-induced esophageal body contractility using FLIP topography in normal controls.
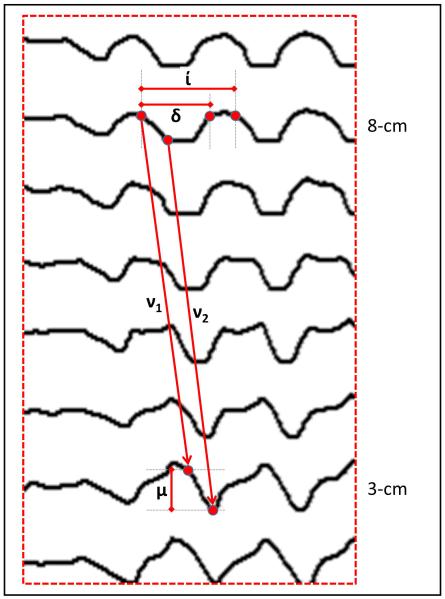
Methods: Ten healthy controls were evaluated during endoscopy with FLIP. During stepwise bag distension, simultaneous intra-bag pressure and luminal diameter measurements were obtained and exported to a MatLab program to generate FLIP topography plots. The distension volume, intra-bag pressure, and maximum esophageal body diameters were measured for the onset and cessation of repetitive antegrade contractions (RACs). Contraction duration, interval, magnitude, and velocity were measured at 8 and 3-cm proximal to the esophagogastric junction.
Key results: Eight of ten subjects demonstrated RACs at a median onset volume of 29 mL (IQR: 25-38.8), median intra-bag pressure of 10.7 mmHg (IQR: 8.6-15.9), and median maximum esophageal body diameter of 18.5 mm (IQR: 17.5-19.6). Cessation of RACs occurred prior to completion of the distension protocol in three of the eight subjects exhibiting RACs. Values of the RAC-associated contractile metrics were also generated to characterize these events.
Conclusions & inferences: Distension-induced esophageal contractions can be assessed utilizing FLIP topography. RACs are a common finding in asymptomatic controls in response to volume distention and have similar characteristics to secondary peristalsis and repetitive rapid swallows.
Keywords: esophageal motility; functional lumen imaging probe; impedance planimetry; secondary peristalsis.
© 2015 John Wiley & Sons Ltd.
Figures
References
-
- McMahon BP, Frokjaer JB, Drewes AM, Gregersen H. A new measurement of oesophago-gastric junction competence. Neurogastroenterology and motility : the official journal of the European Gastrointestinal Motility Society. 2004;16(5):543–6. - PubMed
-
- Rohof WO, Hirsch DP, Kessing BF, Boeckxstaens GE. Efficacy of treatment for patients with achalasia depends on the distensibility of the esophagogastric junction. Gastroenterology. 2012;143(2):328–35. - PubMed
-
- Pandolfino JE, de Ruigh A, Nicodeme F, Xiao Y, Boris L, Kahrilas PJ. Distensibility of the esophagogastric junction assessed with the functional lumen imaging probe (FLIP) in achalasia patients. Neurogastroenterology and motility : the official journal of the European Gastrointestinal Motility Society. 2013;25(6):496–501. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
