

Insulin-independent reversal of type 1 diabetes in nonobese diabetic mice with brown adipose tissue transplant
- PMID: 25898954
- PMCID: PMC4469812
- DOI: 10.1152/ajpendo.00570.2014
Insulin-independent reversal of type 1 diabetes in nonobese diabetic mice with brown adipose tissue transplant
Abstract
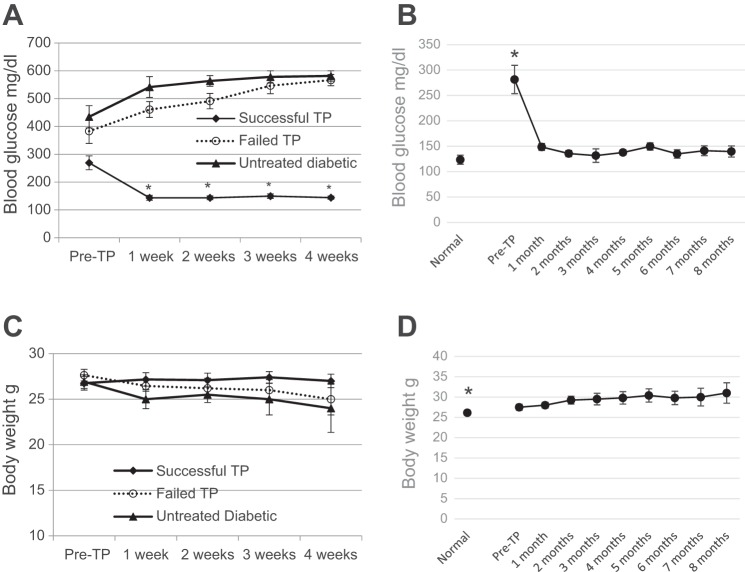
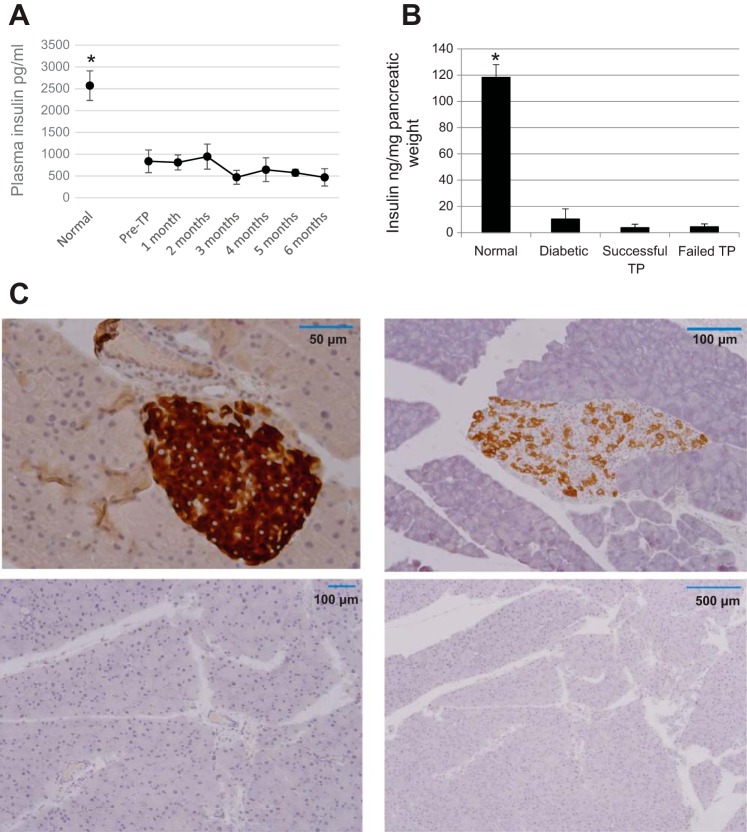
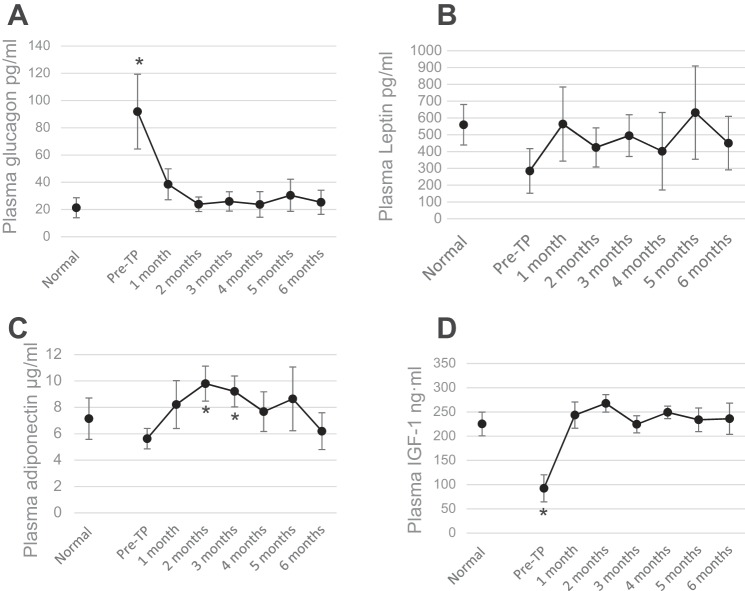
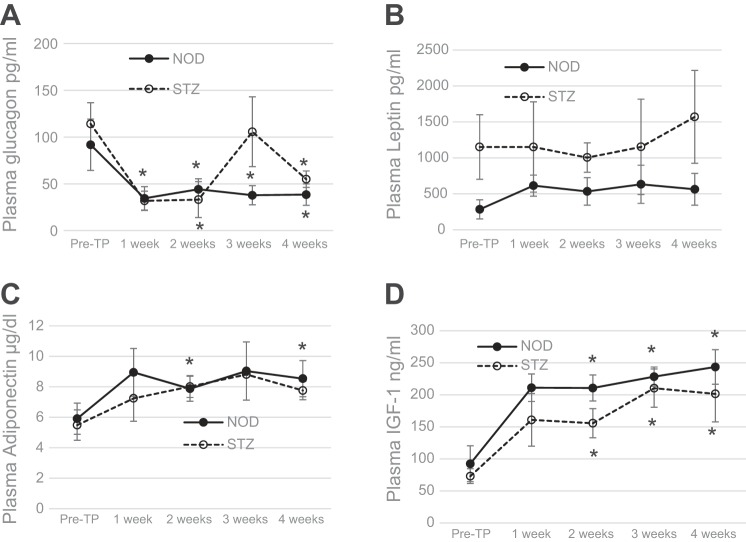
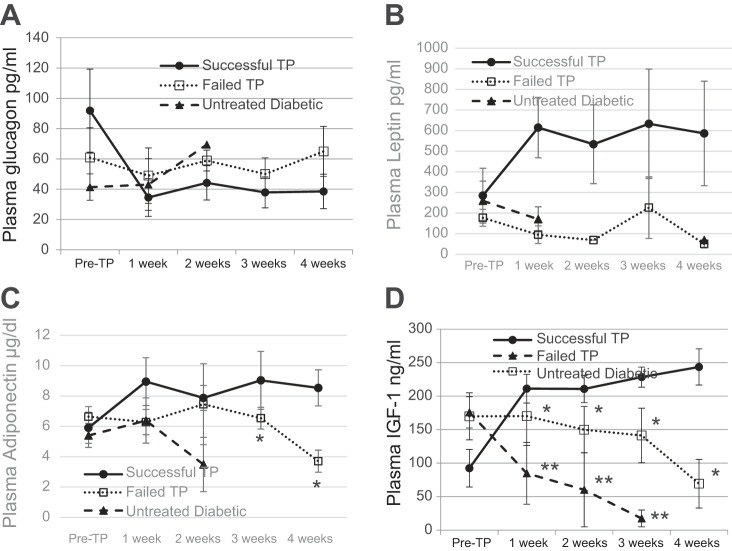
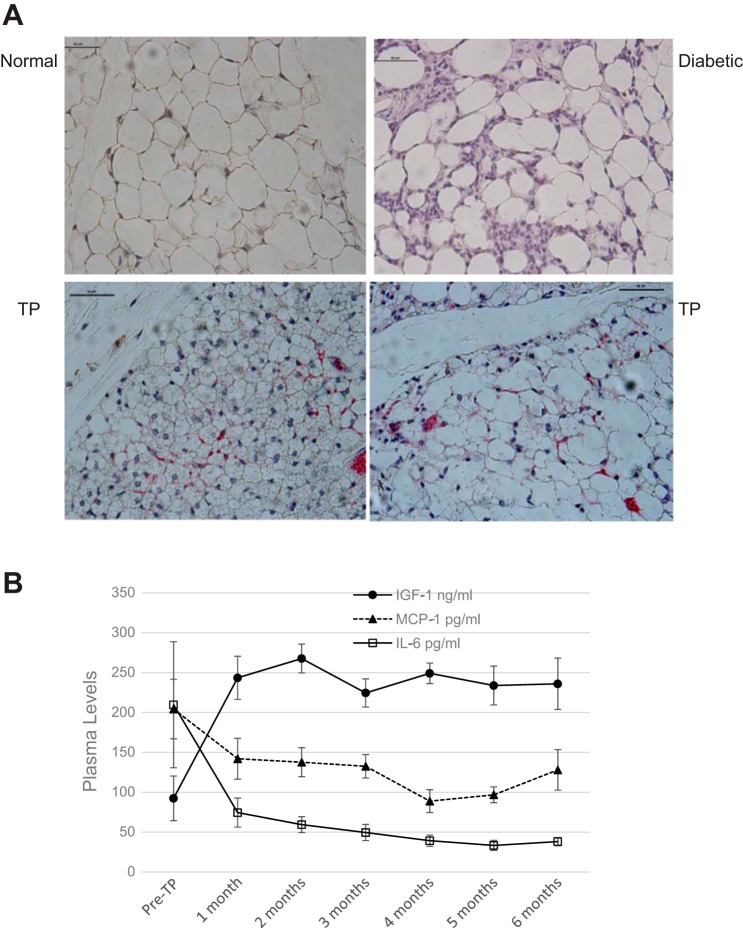
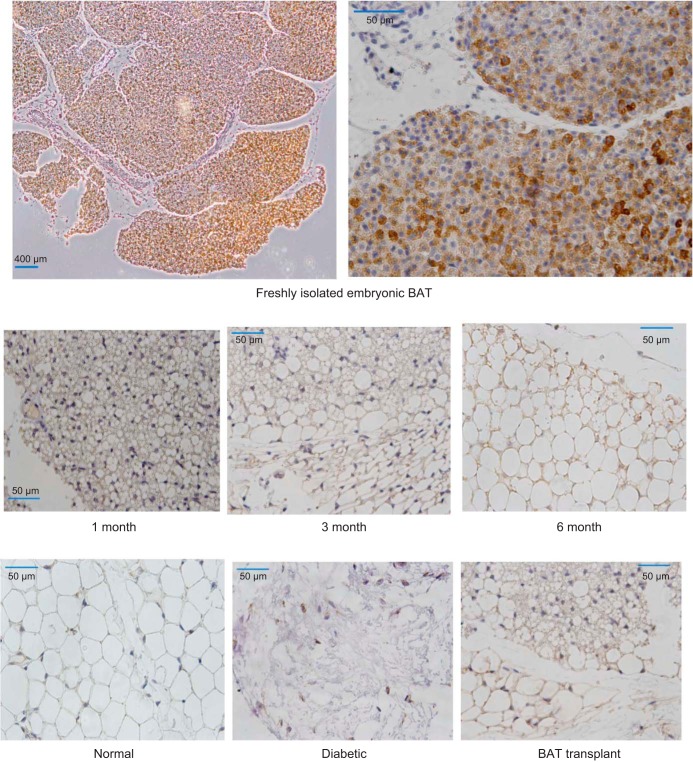
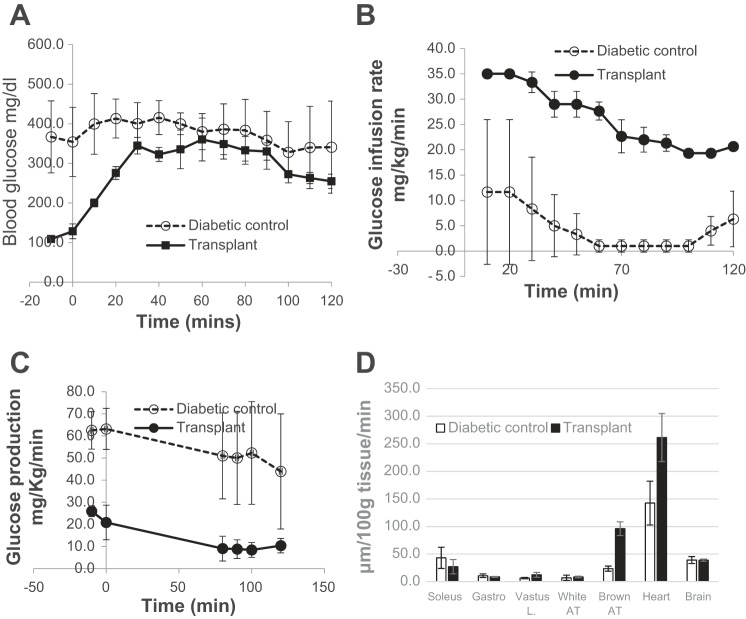
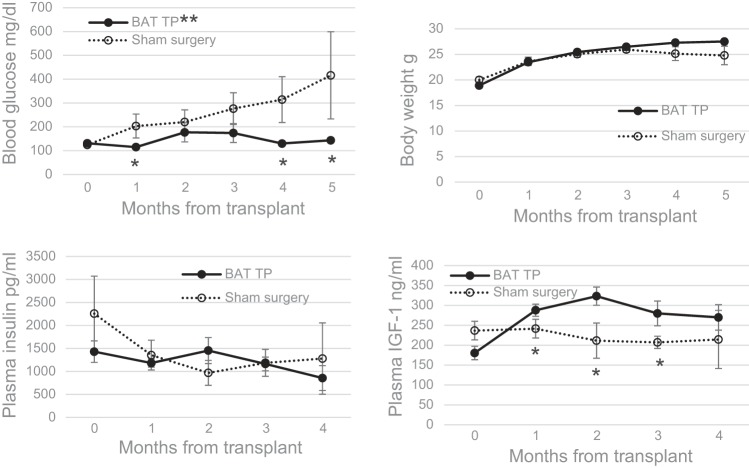
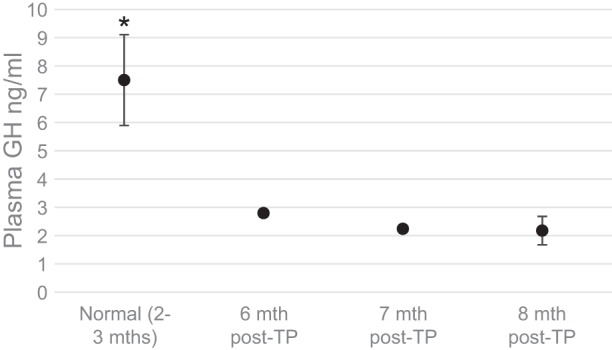
Traditional therapies for type 1 diabetes (T1D) involve insulin replacement or islet/pancreas transplantation and have numerous limitations. Our previous work demonstrated the ability of embryonic brown adipose tissue (BAT) transplants to establish normoglycemia without insulin in chemically induced models of insulin-deficient diabetes. The current study sought to extend the technique to an autoimmune-mediated T1D model and document the underlying mechanisms. In nonobese diabetic (NOD) mice, BAT transplants result in complete reversal of T1D associated with rapid and long-lasting euglycemia. In addition, BAT transplants placed prior to the onset of diabetes on NOD mice can prevent or significantly delay the onset of diabetes. As with streptozotocin (STZ)-diabetic models, euglycemia is independent of insulin and strongly correlates with decrease of inflammation and increase of adipokines. Plasma insulin-like growth factor-I (IGF-I) is the first hormone to increase following BAT transplants. Adipose tissue of transplant recipients consistently express IGF-I compared with little or no expression in controls, and plasma IGF-I levels show a direct negative correlation with glucose, glucagon, and inflammatory cytokines. Adipogenic and anti-inflammatory properties of IGF-I may stimulate regeneration of new healthy white adipose tissue, which in turn secretes hypoglycemic adipokines that substitute for insulin. IGF-I can also directly decrease blood glucose through activating insulin receptor. These data demonstrate the potential for insulin-independent reversal of autoimmune-induced T1D with BAT transplants and implicate IGF-I as a likely mediator in the resulting equilibrium.
Keywords: brown adipose tissue; insulin independent; insulin-like growth factor I; transplantation; type 1 diabetes.
Copyright © 2015 the American Physiological Society.
Figures
References
-
- Acerini CL, Patton CM, Savage MO, Kernell A, Westphal O, Dunger DB. Randomised placebo-controlled trial of human recombinant insulin-like growth factor I plus intensive insulin therapy in adolescents with insulin-dependent diabetes mellitus. Lancet 350: 1199–1204, 1997. - PubMed
-
- Ayala JE, Bracy DP, McGuinness OP, Wasserman DH. Considerations in the design of hyperinsulinemic-euglycemic clamps in the conscious mouse. Diabetes 55: 390–397, 2006. - PubMed
-
- Berg AH, Scherer PE. Adipose tissue, inflammation, and cardiovascular disease. Review Circ Res 96: 939–949, 2005. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials