

Design and validation of a prehospital scale to predict stroke severity: Cincinnati Prehospital Stroke Severity Scale
- PMID: 25899242
- PMCID: PMC4442042
- DOI: 10.1161/STROKEAHA.115.008804
Design and validation of a prehospital scale to predict stroke severity: Cincinnati Prehospital Stroke Severity Scale
Abstract
Background and purpose: We derived and validated the Cincinnati Prehospital Stroke Severity Scale (CPSSS) to identify patients with severe strokes and large vessel occlusion (LVO).
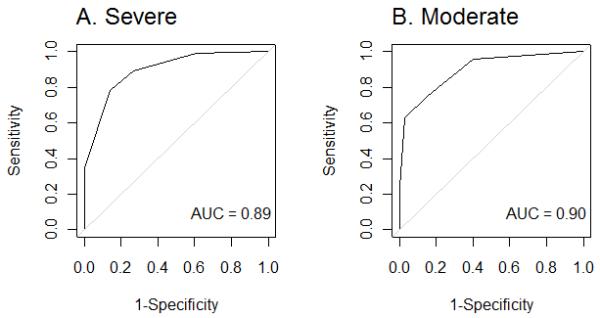
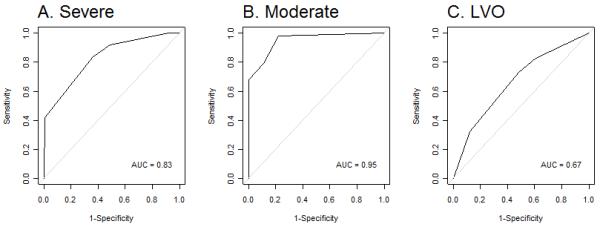
Methods: CPSSS was developed with regression tree analysis, objectivity, anticipated ease in administration by emergency medical services personnel and the presence of cortical signs. We derived and validated the tool using the 2 National Institute of Neurological Disorders and Stroke (NINDS) tissue-type plasminogen activator Stroke Study trials and Interventional Management of Stroke III (IMS III) Trial cohorts, respectively, to predict severe stroke (National Institutes of Health Stroke Scale [NIHSS]≥15) and LVO. Standard test characteristics were determined and receiver operator curves were generated and summarized by the area under the curve.
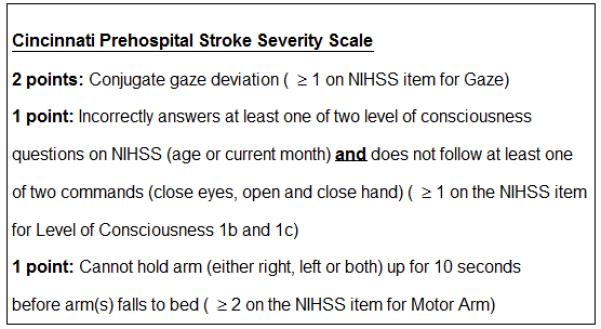
Results: CPSSS score ranges from 0 to 4; composed and scored by individual NIHSS items: 2 points for presence of conjugate gaze (NIHSS≥1); 1 point for presence of arm weakness (NIHSS≥2); and 1 point for presence abnormal level of consciousness commands and questions (NIHSS level of consciousness≥1 each). In the derivation set, CPSSS had an area under the curve of 0.89; score≥2 was 89% sensitive and 73% specific in identifying NIHSS≥15. Validation results were similar with an area under the curve of 0.83; score≥2 was 92% sensitive, 51% specific, a positive likelihood ratio of 3.3, and a negative likelihood ratio of 0.15 in predicting severe stroke. For 222 of 303 IMS III subjects with LVO, CPSSS had an area under the curve of 0.67; a score≥2 was 83% sensitive, 40% specific, positive likelihood ratio of 1.4, and negative likelihood ratio of 0.4 in predicting LVO.
Conclusions: CPSSS can identify stroke patients with NIHSS≥15 and LVO. Prospective prehospital validation is warranted.
Keywords: NIHSS; acute stroke; prehospital emergency care; severe stroke; vessel occlusion.
© 2015 American Heart Association, Inc.
Figures
References
-
- Jauch EC, Saver JL, Adams HP, Jr., Bruno A, Connors JJ, Demaerschalk BM, et al. Guidelines for the early management of patients with acute ischemic stroke: A guideline for healthcare professionals from the american heart association/american stroke association. Stroke; a journal of cerebral circulation. 2013;44:870–947. - PubMed
-
- Diringer MN, Edwards DF. Admission to a neurologic/neurosurgical intensive care unit is associated with reduced mortality rate after intracerebral hemorrhage. Critical care medicine. 2001;29:635–640. - PubMed
-
- Diringer MN, Edwards DF, Aiyagari V, Hollingsworth H. Factors associated with withdrawal of mechanical ventilation in a neurology/neurosurgery intensive care unit. Critical care medicine. 2001;29:1792–1797. - PubMed
-
- Fonarow GC, Pan W, Saver JL, Smith EE, Reeves MJ, Broderick JP, et al. Comparison of 30-day mortality models for profiling hospital performance in acute ischemic stroke with vs without adjustment for stroke severity. Jama. 2012;308:257–264. - PubMed
-
- Meretoja A, Roine RO, Kaste M, Linna M, Roine S, Juntunen M, et al. Effectiveness of primary and comprehensive stroke centers: Perfect stroke: A nationwide observational study from finland. Stroke; a journal of cerebral circulation. 2010;41:1102–1107. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
