

Management Guidelines for Children with Thyroid Nodules and Differentiated Thyroid Cancer
- PMID: 25900731
- PMCID: PMC4854274
- DOI: 10.1089/thy.2014.0460
Management Guidelines for Children with Thyroid Nodules and Differentiated Thyroid Cancer
Abstract
Background: Previous guidelines for the management of thyroid nodules and cancers were geared toward adults. Compared with thyroid neoplasms in adults, however, those in the pediatric population exhibit differences in pathophysiology, clinical presentation, and long-term outcomes. Furthermore, therapy that may be recommended for an adult may not be appropriate for a child who is at low risk for death but at higher risk for long-term harm from overly aggressive treatment. For these reasons, unique guidelines for children and adolescents with thyroid tumors are needed.
Methods: A task force commissioned by the American Thyroid Association (ATA) developed a series of clinically relevant questions pertaining to the management of children with thyroid nodules and differentiated thyroid cancer (DTC). Using an extensive literature search, primarily focused on studies that included subjects ≤18 years of age, the task force identified and reviewed relevant articles through April 2014. Recommendations were made based upon scientific evidence and expert opinion and were graded using a modified schema from the United States Preventive Services Task Force.
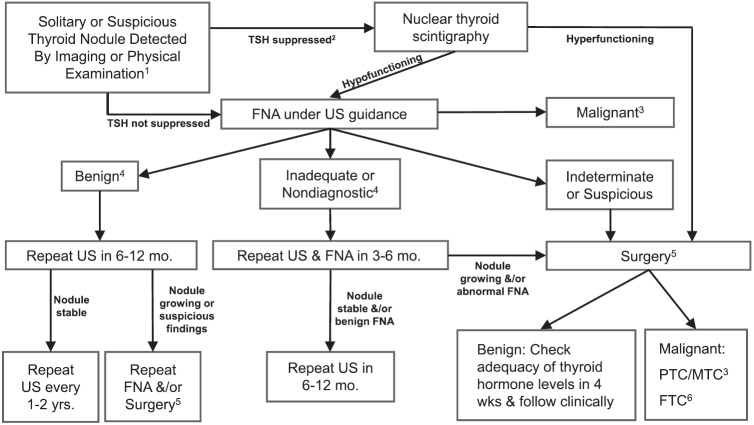
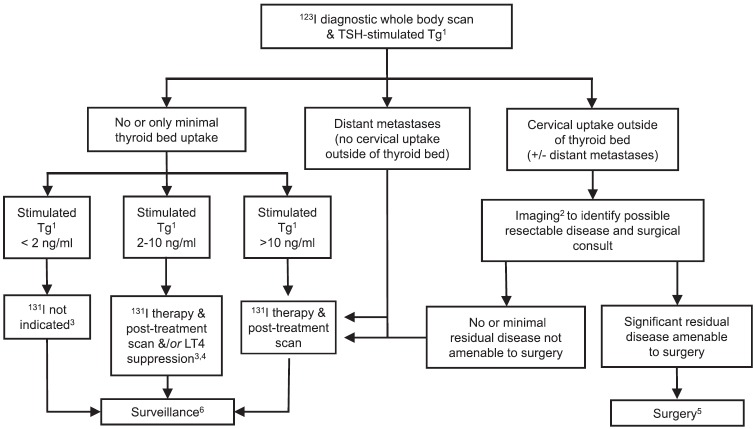
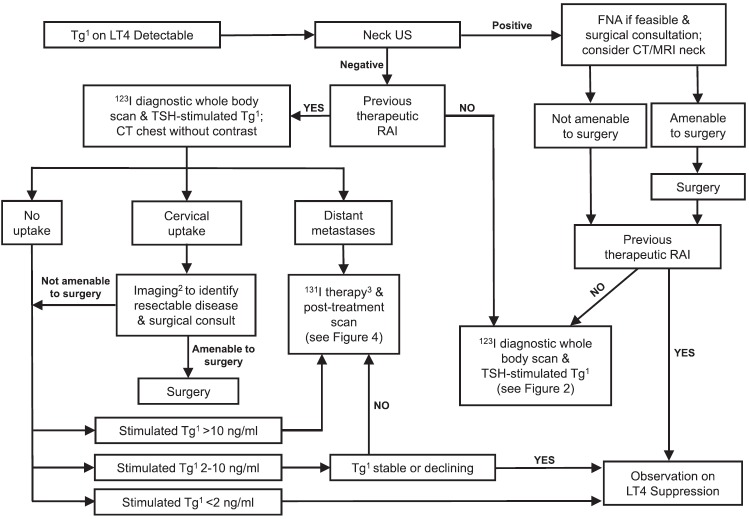
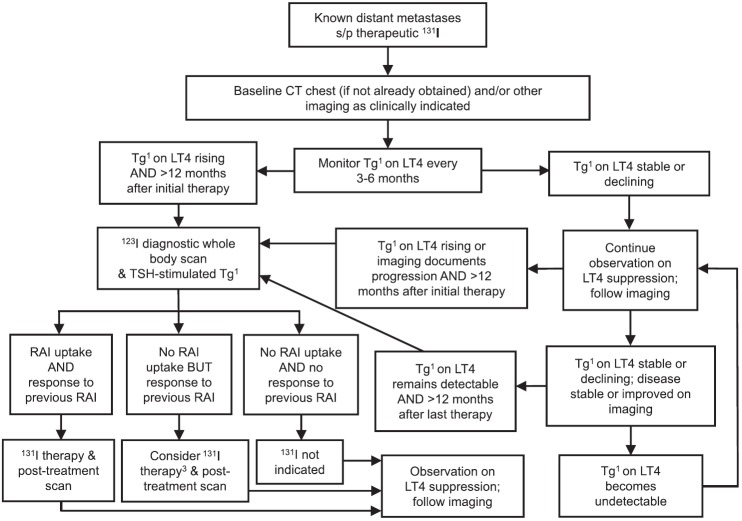
Results: These inaugural guidelines provide recommendations for the evaluation and management of thyroid nodules in children and adolescents, including the role and interpretation of ultrasound, fine-needle aspiration cytology, and the management of benign nodules. Recommendations for the evaluation, treatment, and follow-up of children and adolescents with DTC are outlined and include preoperative staging, surgical management, postoperative staging, the role of radioactive iodine therapy, and goals for thyrotropin suppression. Management algorithms are proposed and separate recommendations for papillary and follicular thyroid cancers are provided.
Conclusions: In response to our charge as an independent task force appointed by the ATA, we developed recommendations based on scientific evidence and expert opinion for the management of thyroid nodules and DTC in children and adolescents. In our opinion, these represent the current optimal care for children and adolescents with these conditions.
Figures
References
-
- Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL, Mandel SJ, Mazzaferri EL, McIver B, Pacini F, Schlumberger M, Sherman SI, Steward DL, Tuttle RM. 2009. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid 19:1167–1214 - PubMed
-
- Cobin RH, Gharib H, Bergman DA, Clark OH, Cooper DS, Daniels GH, Dickey RA, Duick DS, Garber JR, Hay ID, Kukora JS, Lando HM, Schorr AB, Zeiger MA; Thyroid Carcinoma Task Force 2001. AACE/AAES medical/surgical guidelines for clinical practice: management of thyroid carcinoma. American Association of Clinical Endocrinologists. American College of Endocrinology. Endocr Pract 7:202–220 - PubMed
-
- The NCCN Clinical Practice Guidelines in Oncology, Thyroid Carcinoma (Version 2.2013). Available at www.nccn.org/professionals/physician_gls/f_guidelines.asp#site (accessed October3, 2013)
-
- British Thyroid Association, Royal College of Physicians 2007. Guidelines for the Management of Thyroid Cancer. Second edition. Royal College of Physicians, London
-
- Hay ID, Gonzalez-Losada T, Reinalda MS, Honetschlager JA, Richards ML, Thompson GB. 2010. Long-term outcome in 215 children and adolescents with papillary thyroid cancer treated during 1940 through 2008. World J Surg 34:1192–1202 - PubMed
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
