

Preserved Insulin Secretory Capacity and Weight Loss Are the Predominant Predictors of Glycemic Control in Patients With Type 2 Diabetes Randomized to Roux-en-Y Gastric Bypass
- PMID: 25901097
- PMCID: PMC4542441
- DOI: 10.2337/db14-1870
Preserved Insulin Secretory Capacity and Weight Loss Are the Predominant Predictors of Glycemic Control in Patients With Type 2 Diabetes Randomized to Roux-en-Y Gastric Bypass
Abstract
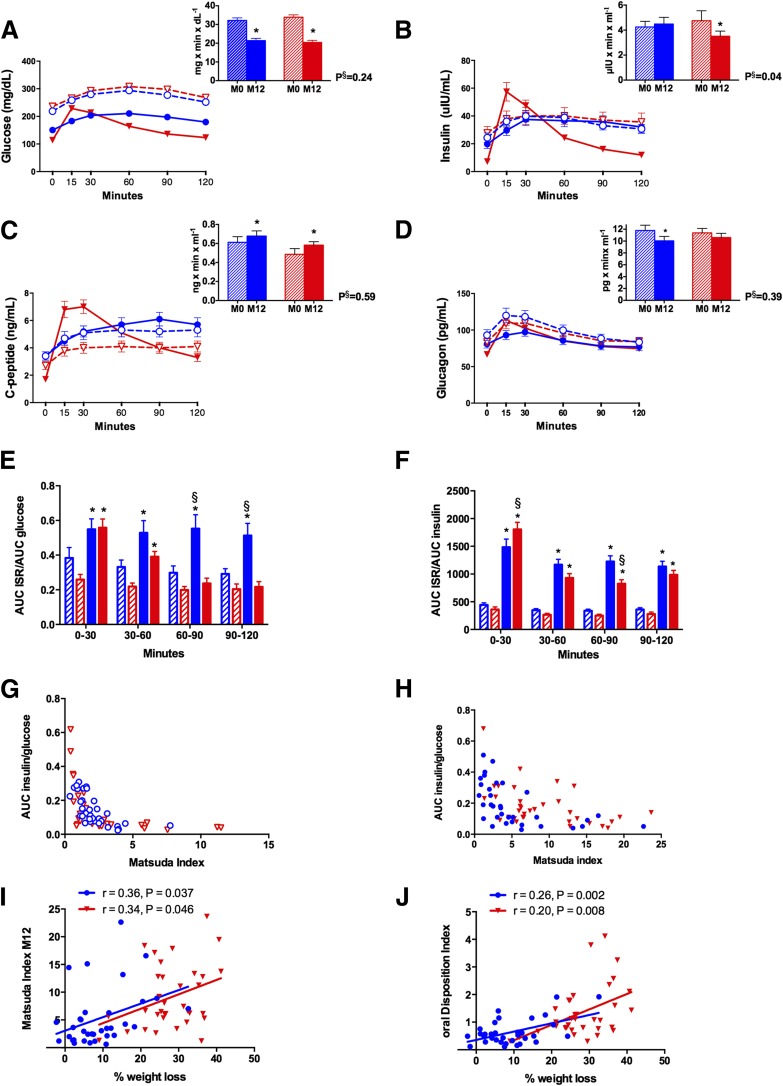
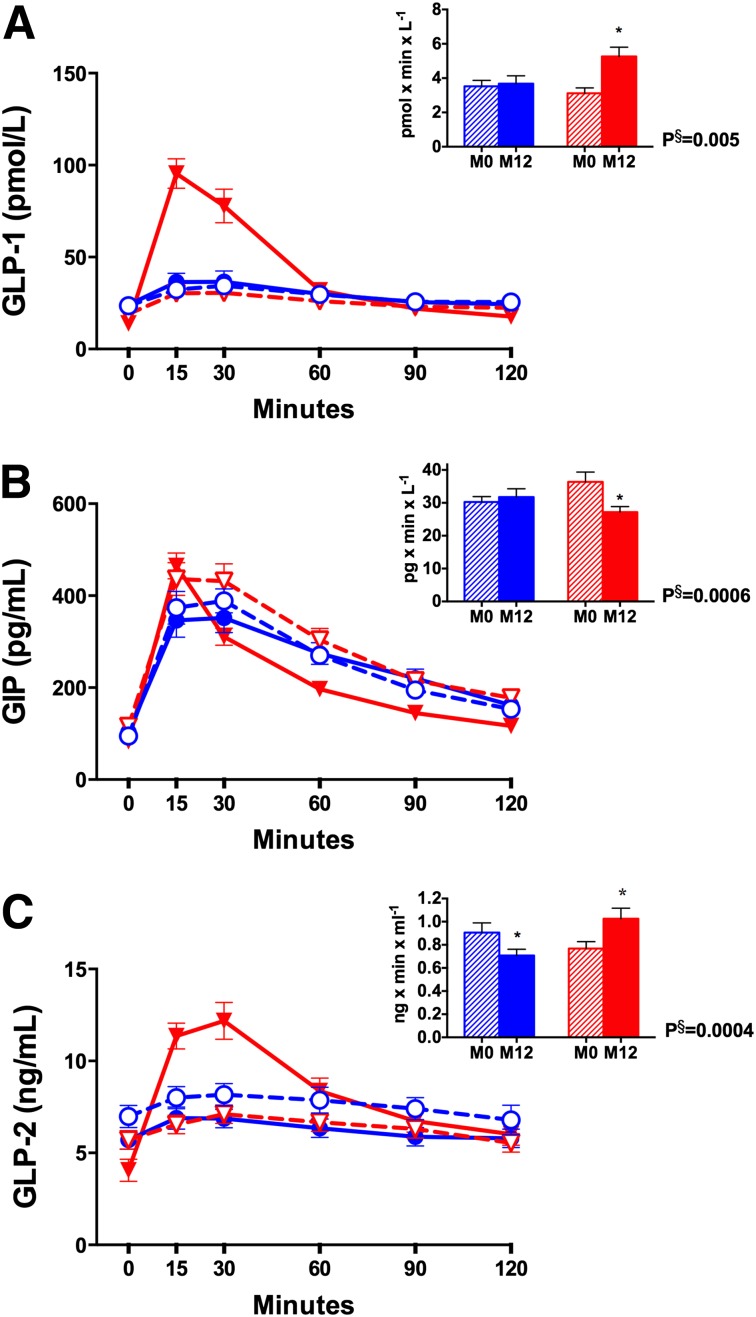
Improvement in type 2 diabetes after Roux-en-Y gastric bypass (RYGB) has been attributed partly to weight loss, but mechanisms beyond weight loss remain unclear. We performed an ancillary study to the Diabetes Surgery Study to assess changes in incretins, insulin sensitivity, and secretion 1 year after randomization to lifestyle modification and intensive medical management (LS/IMM) alone (n = 34) or in conjunction with RYGB (n = 34). The RYGB group lost more weight and had greater improvement in HbA1c. Fasting glucose was lower after RYGB than after LS/IMM, although the glucose area under the curve decreased comparably for both groups. Insulin sensitivity increased in both groups. Insulin secretion was unchanged after LS/IMM but decreased after RYGB, except for a rapid increase during the first 30 min after meal ingestion. Glucagon-like peptide 1 (GLP-1) was substantially increased after RYGB, while gastric inhibitory polypeptide and glucagon decreased. Lower HbA1c was most strongly correlated with the percentage of weight loss for both groups. At baseline, a greater C-peptide index and 90-min postprandial C-peptide level were predictive of lower HbA1c at 1 year after RYGB. β-Cell glucose sensitivity, which improved only after RYGB, and improved disposition index were associated with lower HbA1c in both groups, independent of weight loss. Weight loss and preserved β-cell function both predominantly determine the greatest glycemic benefit after RYGB.
© 2015 by the American Diabetes Association. Readers may use this article as long as the work is properly cited, the use is educational and not for profit, and the work is not altered.
Figures
References
-
- Sjöström L. Bariatric surgery and reduction in morbidity and mortality: experiences from the SOS study. Int J Obes (Lond) 2008;32(Suppl. 7):S93–S97 - PubMed
-
- American Diabetes Association . Standards of medical care in diabetes—2015: summary of revisions. Diabetes Care 2015;38(Suppl.):S4. - PubMed
-
- Dixon JB, Zimmet P, Alberti KG, Rubino F; International Diabetes Federation Taskforce on Epidemiology and Prevention . Bariatric surgery: an IDF statement for obese type 2 diabetes. Arq Bras Endocrinol Metabol 2011;55:367–382 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
