

Costs of testing for ocular Chlamydia trachomatis infection compared to mass drug administration for trachoma in the Gambia: application of results from the PRET study
- PMID: 25901349
- PMCID: PMC4406756
- DOI: 10.1371/journal.pntd.0003670
Costs of testing for ocular Chlamydia trachomatis infection compared to mass drug administration for trachoma in the Gambia: application of results from the PRET study
Abstract
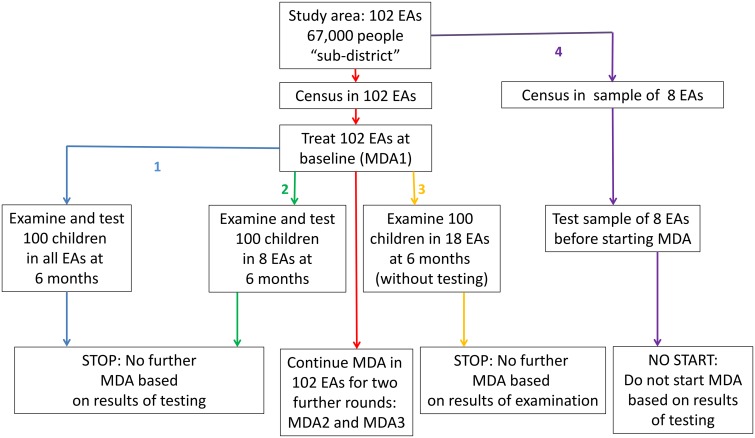
Background: Mass drug administration (MDA) treatment of active trachoma with antibiotic is recommended to be initiated in any district where the prevalence of trachoma inflammation, follicular (TF) is ≥ 10% in children aged 1-9 years, and then to continue for at least three annual rounds before resurvey. In The Gambia the PRET study found that discontinuing MDA based on testing a sample of children for ocular Chlamydia trachomatis(Ct) infection after one MDA round had similar effects to continuing MDA for three rounds. Moreover, one round of MDA reduced disease below the 5% TF threshold. We compared the costs of examining a sample of children for TF, and of testing them for Ct, with those of MDA rounds.
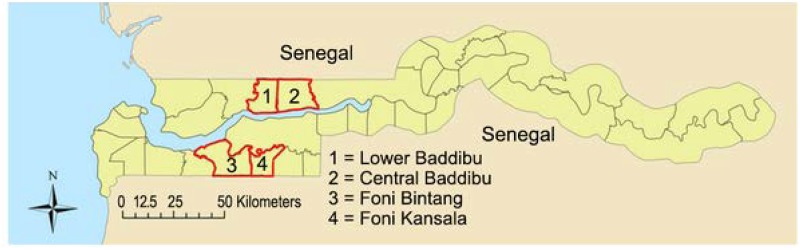
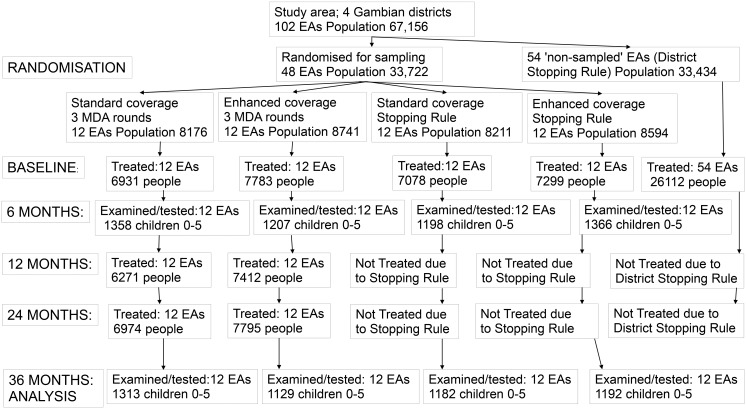
Methods: The implementation unit in PRET The Gambia was a census enumeration area (EA) of 600-800 people. Personnel, fuel, equipment, consumables, data entry and supervision costs were collected for census and treatment of a sample of EAs and for the examination, sampling and testing for Ct infection of 100 individuals within them. Programme costs and resource savings from testing and treatment strategies were inferred for the 102 EAs in the study area, and compared.
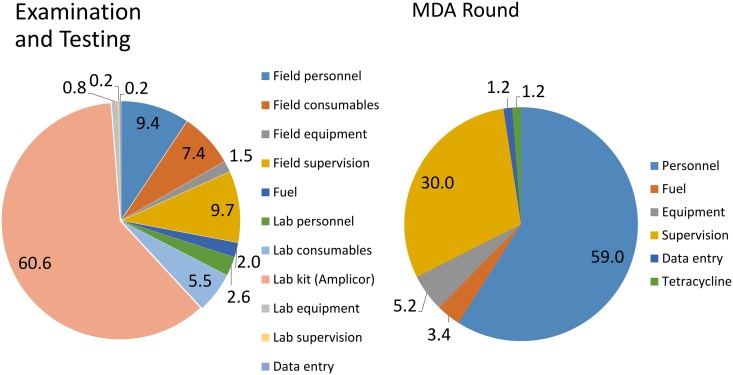
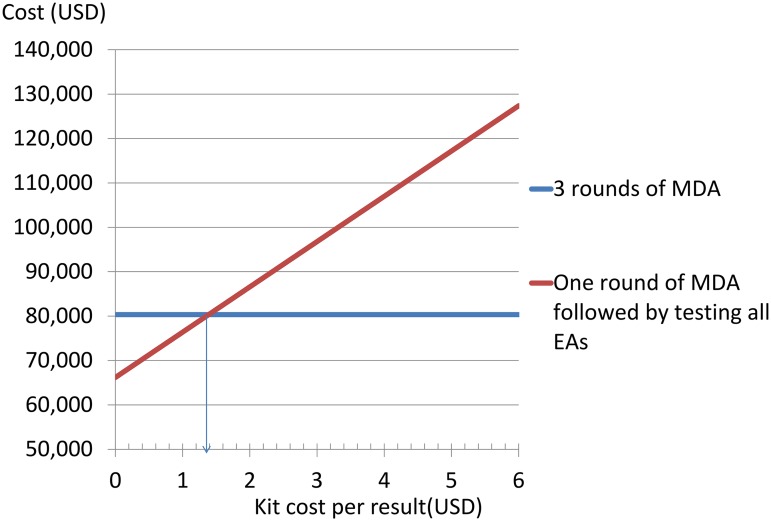
Results: Census costs were $103.24 per EA plus initial costs of $108.79. MDA with donated azithromycin cost $227.23 per EA. The mean cost of examining and testing 100 children was $796.90 per EA, with Ct testing kits costing $4.80 per result. A strategy of testing each EA for infection is more expensive than two annual rounds of MDA unless the kit cost is less than $1.38 per result. However stopping or deciding not to initiate treatment in the study area based on testing a sample of EAs for Ct infection (or examining children in a sample of EAs) creates savings relative to further unnecessary treatments.
Conclusion: Resources may be saved by using tests for chlamydial infection or clinical examination to determine that initial or subsequent rounds of MDA for trachoma are unnecessary.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Frick KD, Hanson CL, Jacobson GA (2003) Global burden of trachoma and economics of the disease. Am J Trop Med Hyg 69: 1–10. - PubMed
-
- Burton MJ, Holland MJ, Makalo P, Aryee EA, Alexander ND, Sillah A et al. (2005) Re-emergence of Chlamydia trachomatis infection after mass antibiotic treatment of a trachoma-endemic Gambian community: a longitudinal study. Lancet 365: 1321–1328. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
