

Chronic gastritis
- PMID: 25901896
- PMCID: PMC4673514
- DOI: 10.3109/00365521.2015.1019918
Chronic gastritis
Abstract
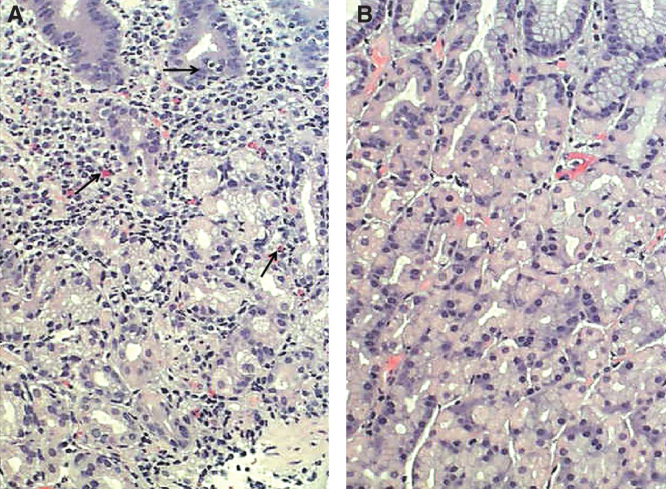
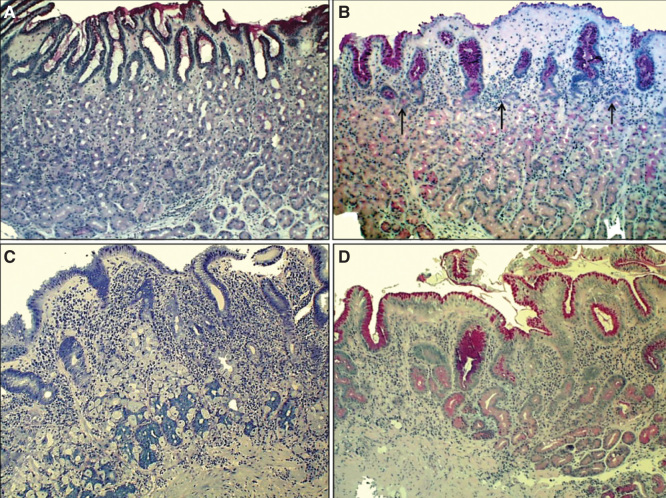
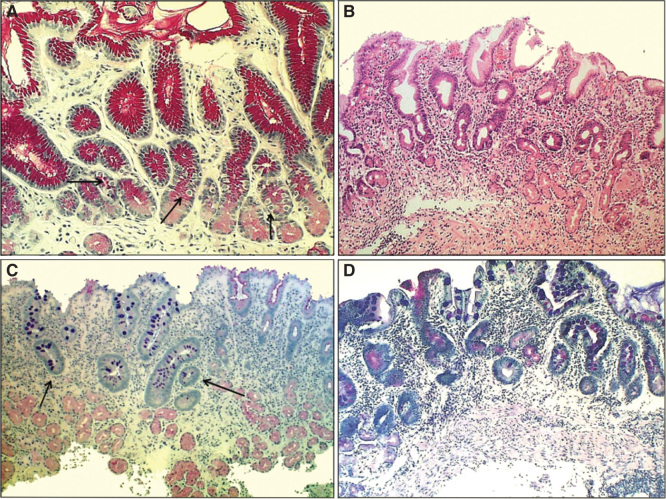
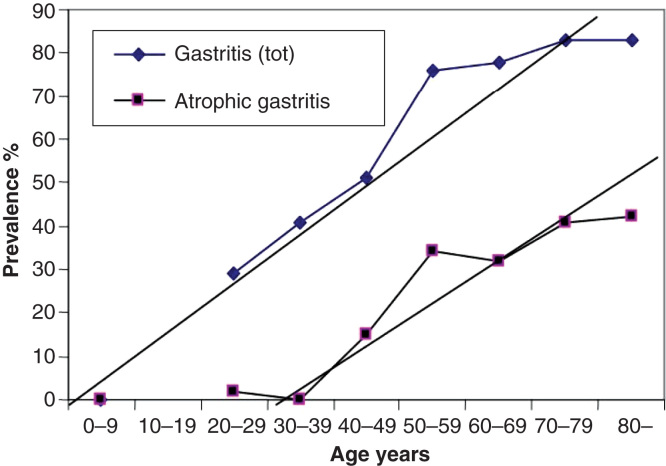
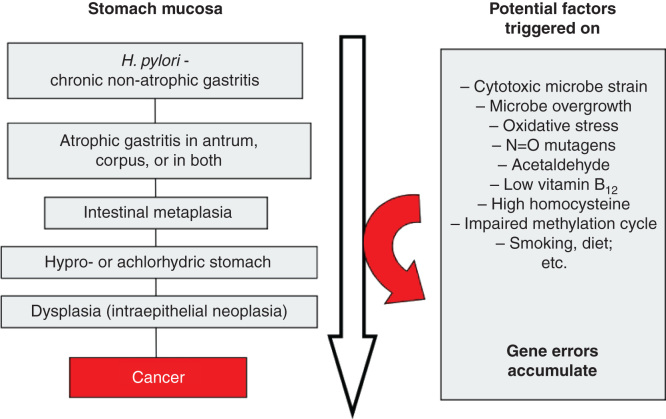
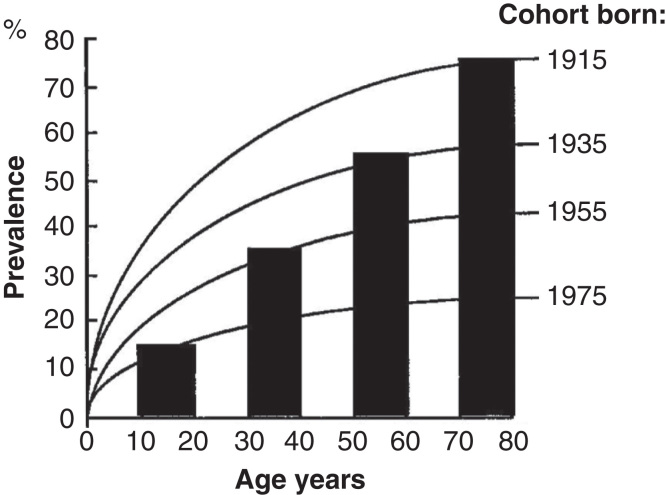
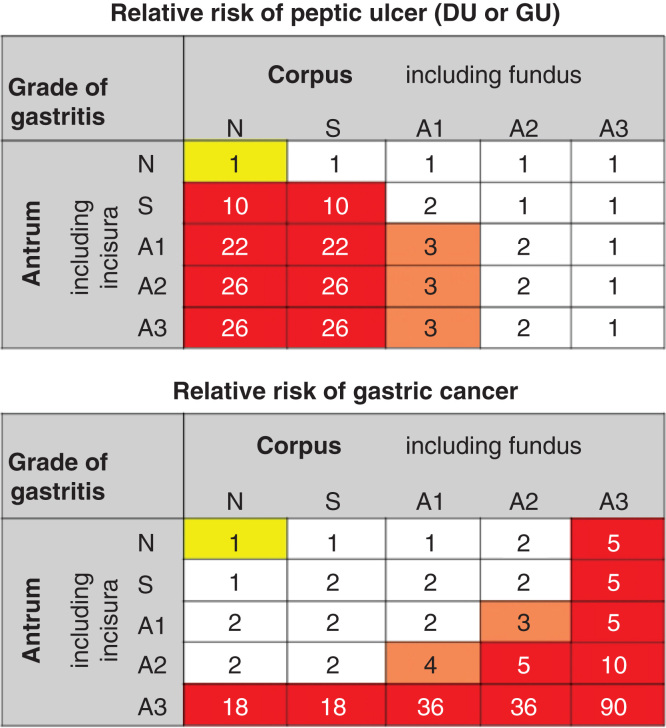
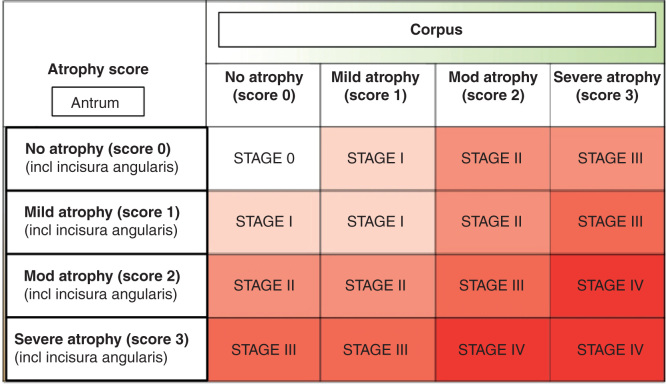
Prevalence of chronic gastritis has markedly declined in developed populations during the past decades. However, chronic gastritis is still one of the most common serious pandemic infections with such severe killing sequelae as peptic ulcer or gastric cancer. Globally, on average, even more than half of people may have a chronic gastritis at present. Helicobacter pylori infection in childhood is the main cause of chronic gastritis, which microbial origin is the key for the understanding of the bizarre epidemiology and course of the disease. A life-long and aggressive inflammation in gastritis results in destruction (atrophic gastritis) of stomach mucosa with time (years and decades). The progressive worsening of atrophic gastritis results subsequently in dysfunctions of stomach mucosa. Atrophic gastritis will finally end up in a permanently acid-free stomach in the most extreme cases. Severe atrophic gastritis and acid-free stomach are the highest independent risk conditions for gastric cancer known so far. In addition to the risks of malignancy and peptic ulcer, acid-free stomach and severe forms of atrophic gastritis may associate with failures in absorption of essential vitamins, like vitamin B12, micronutrients (like iron, calcium, magnesium and zinc), diet and medicines.
Keywords: Helicobacter pylori; gastric cancer; gastritis; peptic ulcer.
Figures
References
-
- Schindler R. Chronic gastritis. Klin Wochenschr. 1966;44:601–12. - PubMed
-
- Siurala M. The story of gastritis. Scand J Gastroenterol Suppl. 1991;186:1–3. - PubMed
-
- Telaranta-Keerie A, Kara R, Paloheimo L, Härkönen M, Sipponen P. Prevalence of undiagnosed advanced atrophic corpus gastritis in Finland: an observational study among 4,256 volunteers without specific complaints. Scand J Gastroenterol. 2010;45:1036–41. - PubMed
-
- Price AB. The Sydney System: histological division. J Gastroenterol Hepatol. 1991;6:209–22. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous