

Nomogram to Predict Postoperative Readmission in Patients Who Undergo General Surgery
- PMID: 25902340
- PMCID: PMC4824195
- DOI: 10.1001/jamasurg.2014.4043
Nomogram to Predict Postoperative Readmission in Patients Who Undergo General Surgery
Abstract
Importance: The Centers for Medicare and Medicaid Services have implemented penalties for hospitals with above-average readmission rates under the Hospital Readmissions Reductions Program. These changes will likely be extended to affect postoperative readmissions in the future.
Objectives: To identify variables that place patients at risk for readmission, develop a predictive nomogram, and validate this nomogram.
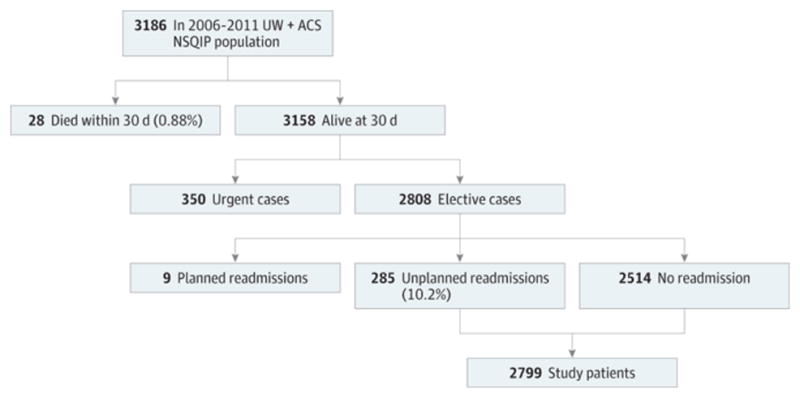
Design, setting, and participants: Retrospective review and prospective validation of a predictive nomogram. A predictive nomogram was developed with the linear predictor method using the American College of Surgeons National Surgical Quality Improvement Program database paired with institutional billing data for patients who underwent nonemergent inpatient general surgery procedures. The nomogram was developed from August 1, 2006, through December 31, 2011, in 2799 patients and prospectively validated from November 1, 2013, through December 19, 2013, in 255 patients at a single academic institution. Area under the curve and positive and negative predictive values were calculated.
Main outcomes and measures: The outcome of interest was readmission within 30 days of discharge following an index hospitalization for a surgical procedure.
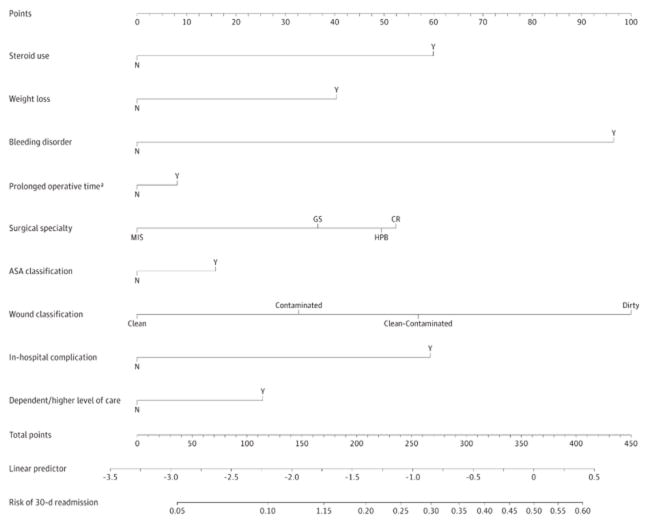
Results: Bleeding disorder (odds ratio, 2.549; 95% CI, 1.464-4.440), long operative time (odds ratio, 1.601; 95% CI, 1.186-2.160), in-hospital complications (odds ratio, 16.273; 95% CI, 12.028-22.016), dependent functional status, and the need for a higher level of care at discharge (odds ratio, 1.937; 95% CI, 1.176-3.190) were independently associated with readmission. The nomogram accurately predicted readmission (C statistic = 0.756) in a prospective evaluation. The negative predictive value was 97.9% in the prospective validation, while the positive predictive value was 11.1%.
Conclusions and relevance: Development of an online calculator using this predictive model will allow us to identify patients who are at high risk for readmission at the time of discharge. Patients with increased risk may benefit from more intensive postoperative follow-up in the outpatient setting.
Conflict of interest statement
The authors have no other conflicts of interest to report.
Figures
Comment in
-
Putting Predictions to the Test.JAMA Surg. 2015 Jun;150(6):511. doi: 10.1001/jamasurg.2015.0417. JAMA Surg. 2015. PMID: 25901474 No abstract available.
-
Some Important Deficiencies in the Development, Validation, and Reporting of a Prediction Model.JAMA Surg. 2015 Sep;150(9):915. doi: 10.1001/jamasurg.2015.1652. JAMA Surg. 2015. PMID: 26200438 No abstract available.
-
Some Important Deficiencies in the Development, Validation, and Reporting of a Prediction Model-Reply.JAMA Surg. 2015 Sep;150(9):915-6. doi: 10.1001/jamasurg.2015.1655. JAMA Surg. 2015. PMID: 26200594 No abstract available.
References
-
- Podulka J, Barrett M, Jiang HJ, Steiner C. 30-Day Readmissions following Hospitalizations for Chronic vs. Acute Conditions, 2008: Statistical Brief #127. 2006 - PubMed
-
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360(14):1418–28. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
