

Prognostic capabilities of coronary computed tomographic angiography before non-cardiac surgery: prospective cohort study
- PMID: 25902738
- PMCID: PMC4413859
- DOI: 10.1136/bmj.h1907
Prognostic capabilities of coronary computed tomographic angiography before non-cardiac surgery: prospective cohort study
Abstract
Objectives: To determine if coronary computed tomographic angiography enhances prediction of perioperative risk in patients before non-cardiac surgery and to assess the preoperative coronary anatomy in patients who experience a myocardial infarction after non-cardiac surgery.
Design: Prospective cohort study.
Setting: 12 centers in eight countries.
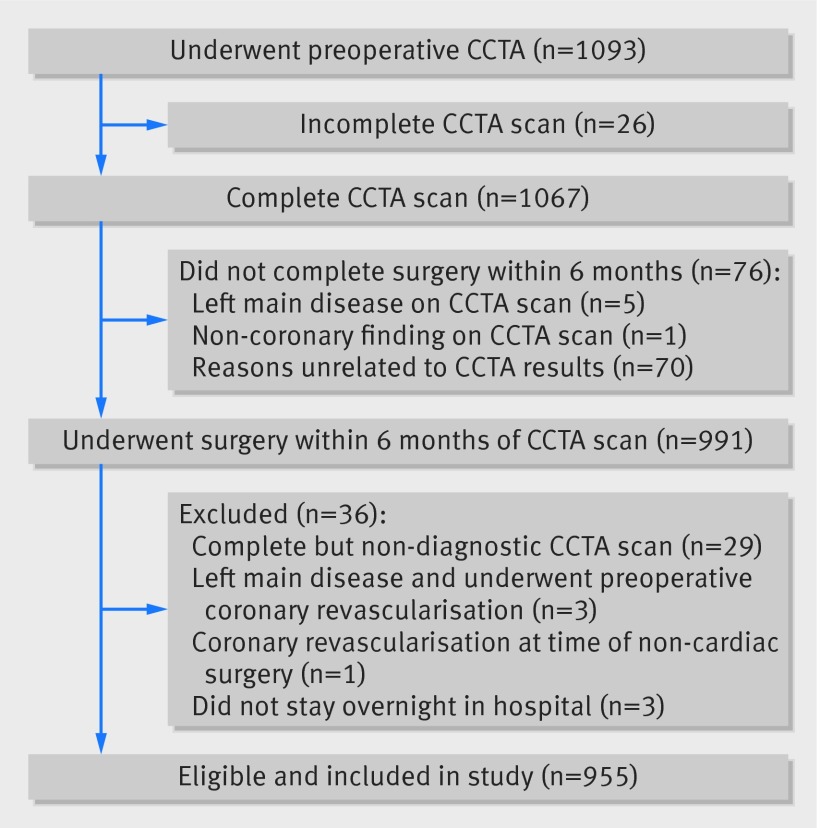
Participants: 955 patients with, or at risk of, atherosclerotic disease who underwent non-cardiac surgery.
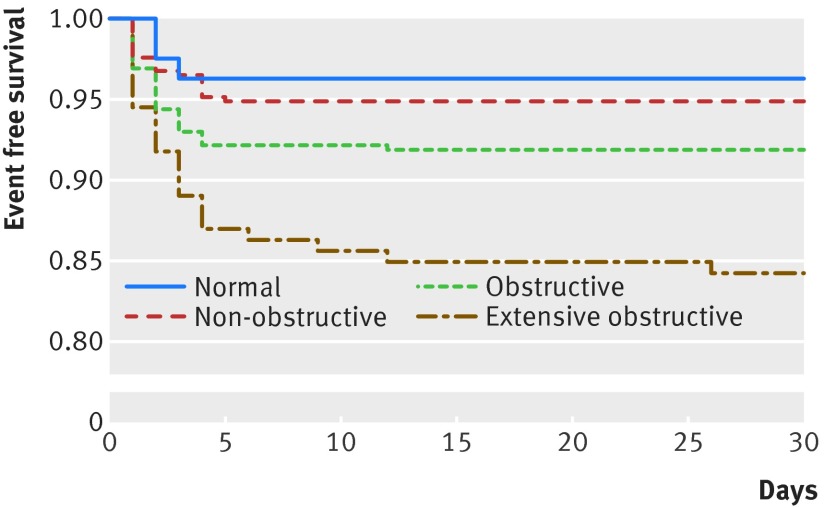
Interventions: Coronary computed tomographic angiography was performed preoperatively; clinicians were blinded to the results unless left main disease was suspected. Results were classified as normal, non-obstructive (<50% stenosis), obstructive (one or two vessels with ≥ 50% stenosis), or extensive obstructive (≥ 50% stenosis in two vessels including the proximal left anterior descending artery, three vessels, or left main).
Main outcome measure: Composite of cardiovascular death and non-fatal myocardial infarction within 30 days after surgery (primary outcome). This was the dependent variable in Cox regression. The independent variables were scores on the revised cardiac risk index and findings on coronary computed tomographic angiography.
Results: The primary outcome occurred in 74 patients (8%). The model that included both scores on the revised cardiac risk index and findings on coronary computed tomographic angiography showed that coronary computed tomographic angiography provided independent prognostic information (P=0.014; C index=0.66). The adjusted hazard ratios were 1.51 (95% confidence interval 0.45 to 5.10) for non-obstructive disease; 2.05 (0.62 to 6.74) for obstructive disease; and 3.76 (1.12 to 12.62) for extensive obstructive disease. For the model with coronary computed tomographic angiography compared with the model based on the revised cardiac risk index alone, with 30 day risk categories of <5%, 5-15%, and >15% for the primary outcome, the results of risk reclassification indicate that in a sample of 1000 patients that coronary computed tomographic angiography would have resulted appropriately in 17 net patients receiving a higher risk estimation among the 77 patients who would have experienced the primary outcome (P<0.001). Coronary computed tomographic angiography, however, would have resulted inappropriately in 98 net patients receiving a higher risk estimation, among the 923 patients who would not have experienced the primary outcome (P<0.001). Among patients who had a perioperative myocardial infarction, preoperative coronary anatomy showed extensive obstructive disease in 31% (22/71), obstructive disease in 41% (29/71), non-obstructive disease in 24% (17/71), and normal findings in 4% (3/71).
Conclusions: Though findings on coronary computed tomographic angiography can improve estimation of risk for patients who will experience perioperative cardiovascular death or myocardial infarction, findings are more than five times as likely to lead to an inappropriate overestimation of risk among patients who will not experience these outcomes. Perioperative myocardial infarction occurs across the spectrum of coronary artery disease, suggesting that there could be several pathophysiologic mechanisms.
© Sheth et al 2015.
Conflict of interest statement
Competing interests: All authors have completed the Unified Competing Interest form at
Figures
References
-
- Devereaux PJ, Chan MT, Alonso-Coello P, et al. Vascular Events In Noncardiac Surgery Patients Cohort Evaluation Study I, Association between postoperative troponin levels and 30-day mortality among patients undergoing noncardiac surgery. JAMA 2012;307:2295-304. - PubMed
-
- Devereaux PJ, Chan M, Eikelboom J. Major vascular complications in patients undergoing non-cardiac surgery: the magnitude of the problem, risk prediction, surveillance, and prevention. In: Yusuf S, Cairns J, Camm AJ, et al, ed. Evidence based cardiology. 3rd ed. BMJ Books, 2009:47-62.
-
- Kristensen SD, Knuuti J, Saraste A, et al. 2014 ESC/ESA Guidelines on non-cardiac surgery: cardiovascular assessment and management: the joint task force on non-cardiac surgery: cardiovascular assessment and management of the European Society of Cardiology (ESC) and the European Society of Anaesthesiology (ESA). Eur Heart J 2014;35:2383-431. - PubMed
-
- Fleisher LA, Fleischmann KE, Auerbach AD, et al. 2014 ACC/AHA guideline on perioperative cardiovascular evaluation and management of patients undergoing noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines. J Am Coll Cardiol 2014;64:e77-137. - PubMed
-
- Chan A, Livingstone D, Tu J. The Goldman and Detsky cardiac-risk indices: Do they work in patients undergoing hip-fracture surgery? Annals RCPSC 1999;32:337-41.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical