

Is maximum primary tumor diameter still a prognostic factor in patients with nasopharyngeal carcinoma treated using intensity-modulated radiotherapy?
- PMID: 25903652
- PMCID: PMC4406035
- DOI: 10.1186/s12885-015-1288-8
Is maximum primary tumor diameter still a prognostic factor in patients with nasopharyngeal carcinoma treated using intensity-modulated radiotherapy?
Abstract
Background: Intensity-modulated radiation therapy (IMRT) has represented a technical milestone that has facilitated the clinical implementation. The purpose of this study was to evaluate the prognostic value of maximum primary tumor diameter (MPTD) in patients with nasopharyngeal carcinoma (NPC) treated using IMRT.
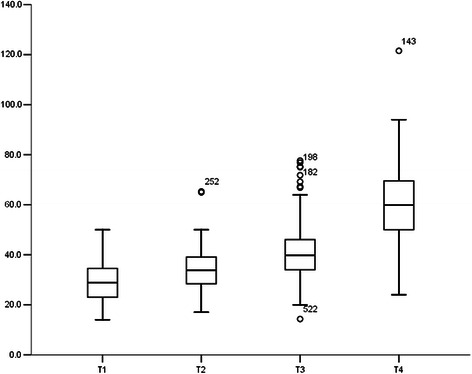
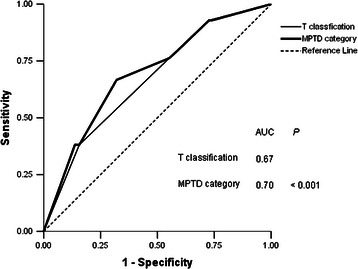
Methods: Five-hundred and sixty-six patients with non-metastatic, histologically-confirmed NPC were retrospectively reviewed. MPTD was measured using magnetic resonance imaging (MRI). All patients were treated using IMRT; 87.5% (456/521) of patients with Stage T3-T4/N1-N3 disease also received cisplatin-based chemotherapy. Receiver operating characteristic (ROC) curves were used to identify the optimal MPTD cut-off point and examine the prognostic value of combining MPTD with the current T classification criteria.
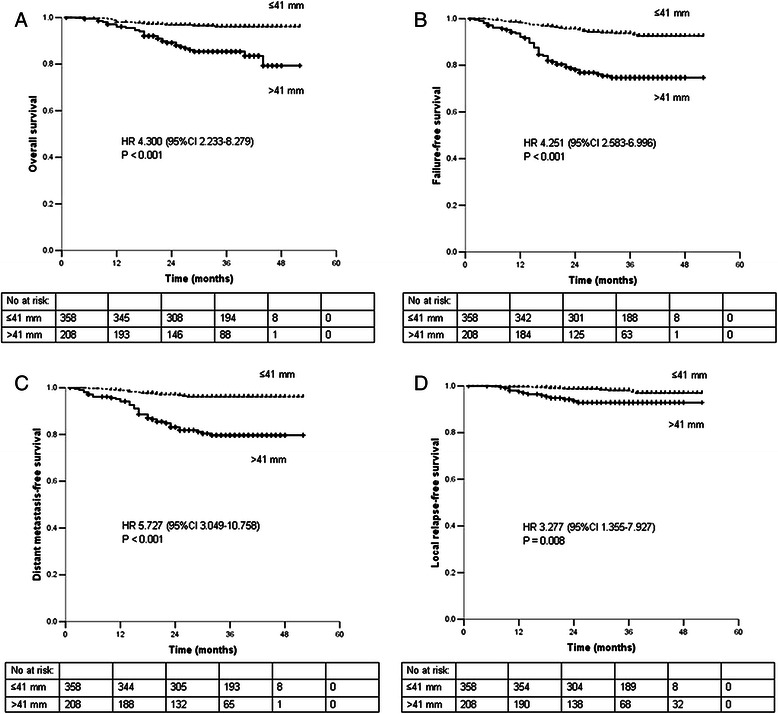
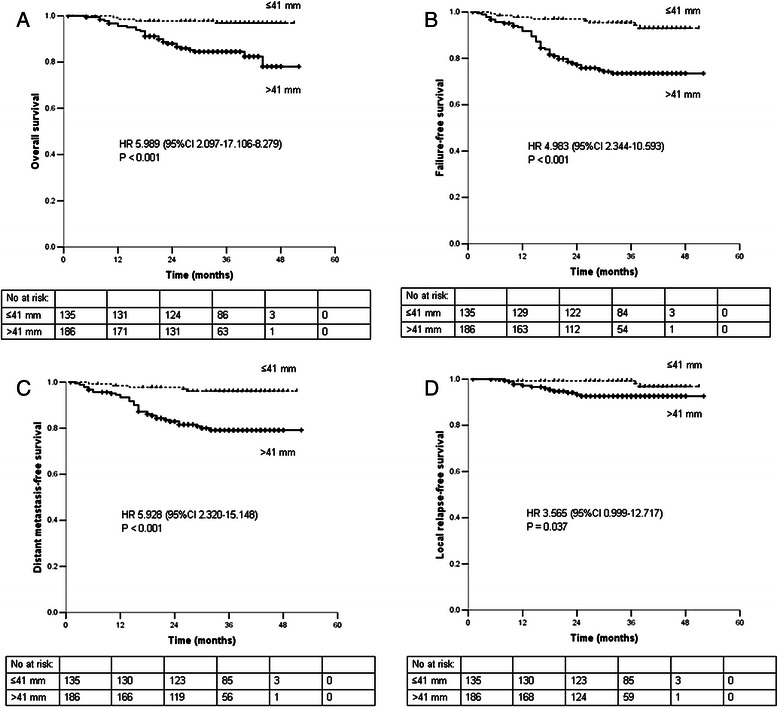
Results: Median follow-up for all patients was 36 months (range, 1-52 months). The 3-year overall survival (OS), failure-free survival (FFS), distant metastasis-free survival (DMFS), and local relapse-free survival (LRFS) rates for patients with a MPTD ≤41 vs. >41 mm were 96.1% vs. 85.4%, 93.7% vs. 74.7%, 96.1% vs. 79.7%, and 98.1% vs. 92.9%, respectively (all P < 0.05). In multivariate analysis, MPTD was an independent prognostic factor for OS, FFS, DMFS and LRFS in all patients (all P < 0.05). Among stage T3-T4 patients, the 3-year OS, FFS, DMFS, and LRFS rates for patients with a MPTD ≤41 vs. >41 mm were 96.9% vs. 84.5%, 95.4% vs. 73.5%, 96.1% vs. 79.2%, and 99.3% vs. 92.6%, respectively (all P < 0.05). In multivariate analysis, MPTD was also an independent prognostic factor for OS, FFS and DMFS in stage T3-T4 patients (all P < 0.05), and the difference in LRFS was almost statistically significant (P = 0.05). ROC curves verified that inclusion of MPTD improved the predictive value of the current T classification criteria (P < 0.001).
Conclusions: MPTD was an independent prognostic factor in patients with NPC treated using IMRT, and significantly improved the prognostic value of the current T classification criteria for NPC.
Figures
References
-
- Chen L, Mao YP, Xie FY, Liu LZ, Sun Y, Tian L, et al. The seventh edition of the UICC/AJCC staging system for nasopharyngeal carcinoma is prognostically useful for patients treated with intensity-modulated radiotherapy from an endemic area in China. Radiother Oncol. 2012;104:331–7. doi: 10.1016/j.radonc.2011.10.009. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
