

Molecular heterogeneity assessment by next-generation sequencing and response to gefitinib of EGFR mutant advanced lung adenocarcinoma
- PMID: 25904052
- PMCID: PMC4494974
- DOI: 10.18632/oncotarget.3727
Molecular heterogeneity assessment by next-generation sequencing and response to gefitinib of EGFR mutant advanced lung adenocarcinoma
Abstract
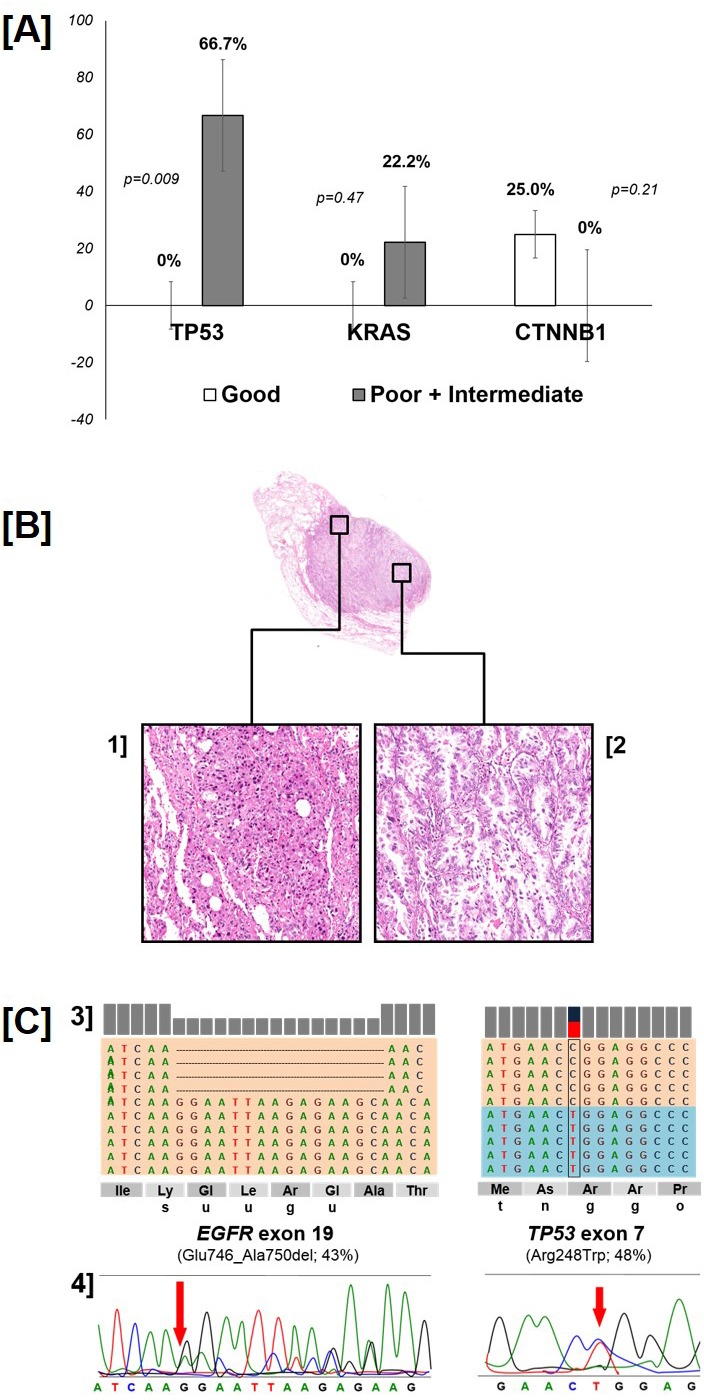
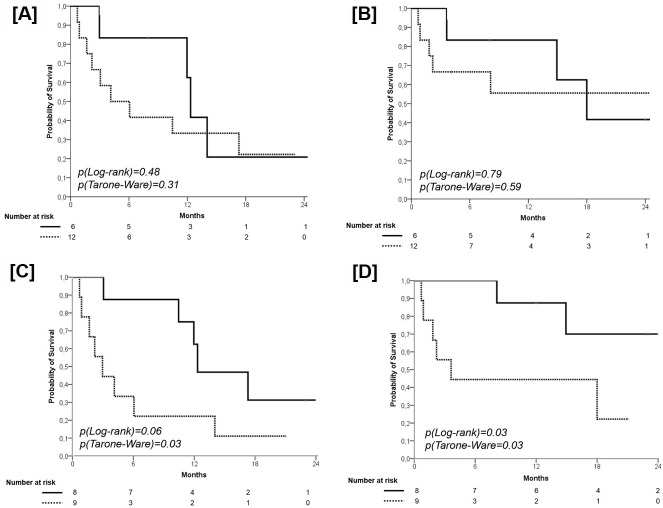
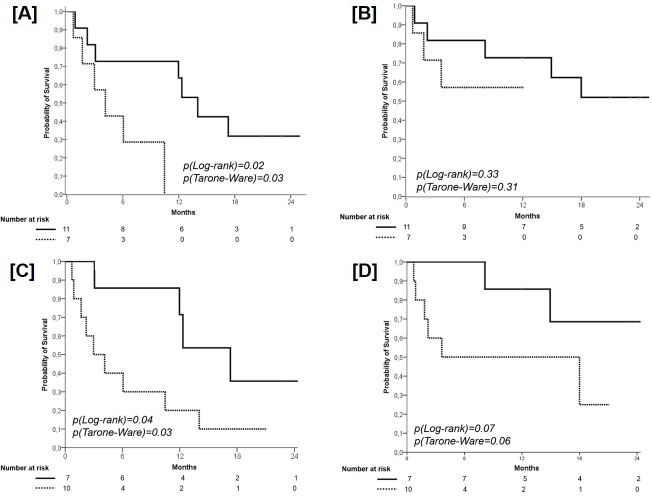
Cancer molecular heterogeneity might explain the variable response of EGFR mutant lung adenocarcinomas to tyrosine kinase inhibitors (TKIs). We assessed the mutational status of 22 cancer genes by next-generation sequencing (NGS) in poor, intermediate or good responders to first-line gefitinib. Clinical outcome was correlated with Additional Coexisting Mutations (ACMs) and the EGFR Proportion of Mutated Alleles (PMA). Thirteen ACMs were found in 10/17 patients: TP53 (n=6), KRAS (n=2), CTNNB1 (n=2), PIK3CA, SMAD4 and MET (n=1 each). TP53 mutations were exclusive of poor/intermediate responders (66.7% versus 0, p=0.009). Presence of ACMs significantly affected both PFS (median 3.0 versus 12.3 months, p=0.03) and survival (3.6 months versus not reached, p=0.03). TP53 mutation was the strongest negative modifier (median PFS 4.0 versus 14.0 months). Higher EGFR PMA was present in good versus poor/intermediate responders. Median PFS and survival were longer in patients with EGFR PMA ≥0.36 (12.0 versus 4.0 months, p=0.31; not reached versus 18.0 months, p=0.59). Patients with an EGFR PMA ≥0.36 and no ACMs fared significantly better (p=0.03), with a trend towards increased survival (p=0.06). Our exploratory data suggest that a quantitative (PMA) and qualitative (ACMs) molecular heterogeneity assessment using NGS might be useful for a better selection of patients.
Keywords: EGFR; gefitinib; lung cancer; next-generation sequencing.
Conflict of interest statement
E.Bria has a consultancy role for Celgene, boards' participation for Novartis, Astra-Zeneca, Pierre-Fabre, and speaker's fee from Pfizer; S.Novello declares boards' participation for Novartis, Astra-Zeneca, MSD, Boehringer Ingelheim, Eli Lilly, Roche and speaker's fee from Pfizer; M. Milella declares boards' participation for Celgene, Astra-Zeneca, Boehringer Ingelheim, and speaker's fee from Pfizer, Novartis, and Celgene; A. Scarpa declares consultancies for Amgen, and boards' participation for Novartis, Sanofi; G.Tortora has consultancy role for Novartis, Pfizer and GSK. No potential conflicts of interest were disclosed by the other authors.
Figures
References
-
- Rosell R, Carcereny E, Gervais R, Vergnenegre A, Massuti B, Felip E, Palmero R, Garcia-Gomez R, Pallares C, Sanchez JM, Porta R, Cobo M, Garrido P, Longo F, Moran T, Insa A, et al. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): a multicentre, open-label, randomised phase 3 trial. Lancet Oncol. 2012;13:239–246. - PubMed
-
- Mitsudomi T, Morita S, Yatabe Y, Negoro S, Okamoto I, Tsurutani J, Seto T, Satouchi M, Tada H, Hirashima T, Asami K, Katakami N, Takada M, Yoshioka H, Shibata K, Kudoh S, et al. Gefitinib versus cisplatin plus docetaxel in patients with non-small-cell lung cancer harbouring mutations of the epidermal growth factor receptor (WJTOG3405): an open label, randomised phase 3 trial. Lancet Oncol. 2010;11:121–128. - PubMed
-
- Maemondo M, Inoue A, Kobayashi K, Sugawara S, Oizumi S, Isobe H, Gemma A, Harada M, Yoshizawa H, Kinoshita I, Fujita Y, Okinaga S, Hirano H, Yoshimori K, Harada T, Ogura T, et al. Gefitinib or chemotherapy for non-small-cell lung cancer with mutated EGFR. N Engl J Med. 2010;362:2380–2388. - PubMed
-
- Sequist LV, Yang JC, Yamamoto N, O'Byrne K, Hirsh V, Mok T, Geater SL, Orlov S, Tsai CM, Boyer M, Su WC, Bennouna J, Kato T, Gorbunova V, Lee KH, Shah R, et al. Phase III study of afatinib or cisplatin plus pemetrexed in patients with metastatic lung adenocarcinoma with EGFR mutations. J Clin Oncol. 2013;31:3327–3334. - PubMed
-
- Pilotto S, Di Maio M, Peretti U, Kinspergher S, Brunelli M, Massari F, Sperduti I, Giannarelli D, De Marinis F, Tortora G, Bria E. Predictors of outcome for patients with lung adenocarcinoma carrying the epidermal growth factor receptor mutation receiving 1st-line tyrosine kinase inhibitors: Sensitivity and meta-regression analysis of randomized trials. Crit Rev Oncol Hematol. 2014;90:135–145. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
