

Trends in myocardial infarction secondary prevention: The National Health and Nutrition Examination Surveys (NHANES), 1999-2012
- PMID: 25904591
- PMCID: PMC4579957
- DOI: 10.1161/JAHA.114.001709
Trends in myocardial infarction secondary prevention: The National Health and Nutrition Examination Surveys (NHANES), 1999-2012
Abstract
Background: Nationally representative data evaluating recent trends and future projections of vascular risk factor treatment and control rates in secondary prevention of ischemic heart disease are sparse.
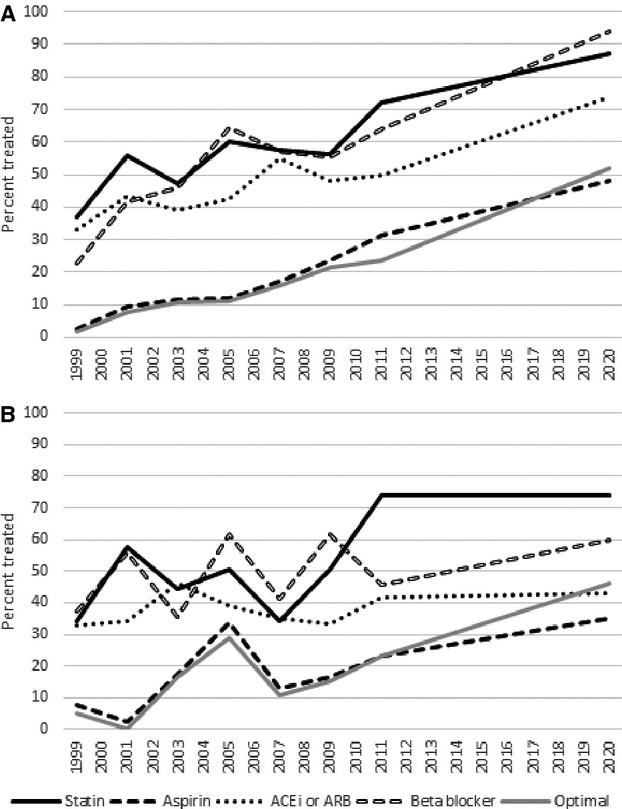
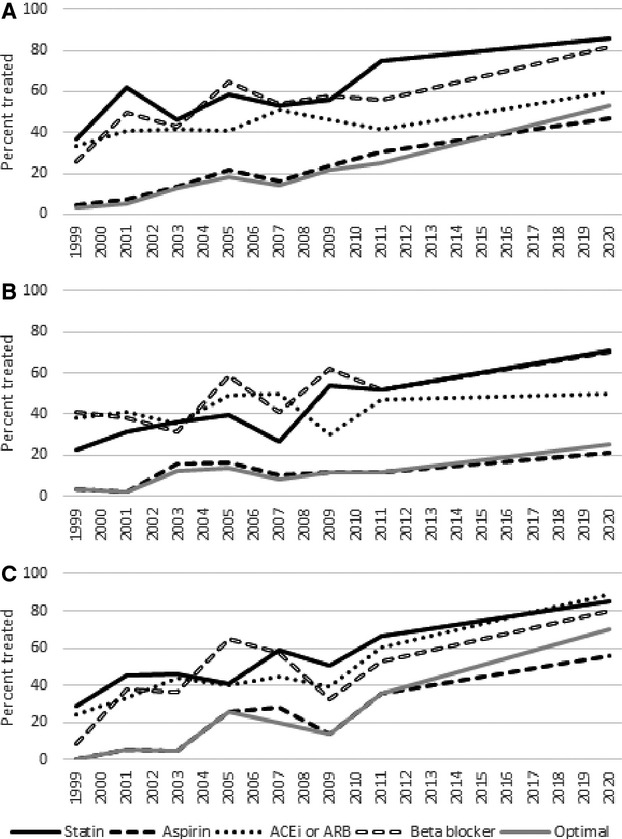
Methods and results: We evaluated sex- and race-stratified cholesterol, blood pressure, and hemoglobin A1c levels and risk factor treatment and control rates in 1580 individuals who self-reported a history of myocardial infarction from The National Health and Nutrition Examination Surveys (NHANES) 1999 to 2012. We used weighted linear regression to estimate time trends and created forward linear projections to 2020. Participants were 30% to 41% women, 73% to 85% white, and had a mean age of 63 to 66 years. Cholesterol treatment rates increased and reached above 80% in men and women by 2011-2012, with significant increases in control rates (as then defined) in men to 85% in 2011-2012, with projections to reach 100% by 2020. Cholesterol treatment rates significantly increased in non-Hispanic whites and Hispanics. Statin use increased significantly to 73% of myocardial infarction survivors by 2011-2012, and aspirin use increased significantly but only to 28% by 2011-2012. There were no changes in blood pressure treatment or control rates by sex, and hypertension treatment increased only in non-Hispanic blacks. Projected hypertension control rates remained suboptimal.
Conclusions: While temporal trends suggest improvements in cholesterol treatment, unchanged treatment and control of blood pressure and persistently low aspirin use represent missed opportunities. Urgent action is needed to improve secondary prevention rates projected by 2020 to reduce recurrent events in this high-risk group.
Keywords: myocardial infarction; secondary prevention; trends.
© 2015 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures
References
-
- Centers for Disease Control and Prevention. Leading causes of death. 2013.
-
- Go AS, Mozaffarian D, Roger VL, Benjamin EJ, Berry JD, Blaha MJ, Dai S, Ford ES, Fox CS, Franco S, Fullerton HJ, Gillespie C, Hailpern SM, Heit JA, Howard VJ, Huffman MD, Judd SE, Kissela BM, Kittner SJ, Lackland DT, Lichtman JH, Lisabeth LD, Mackey RH, Magid DJ, Marcus GM, Marelli A, Matchar DB, McGuire DK, Mohler ER, III, Moy CS, Mussolino ME, Neumar RW, Nichol G, Pandey DK, Paynter NP, Reeves MJ, Sorlie PD, Stein J, Towfighi A, Turan TN, Virani SS, Wong ND, Woo D, Turner MB. Heart disease and stroke statistics—2014 update. Circulation. 2014; 129:e28-e292. - PMC - PubMed
-
- Benjamin SM, Geiss LS, Pan L, Engelgau MM, Greenlund KJ. Self‐reported heart disease and stroke among adults with and without diabetes—United States, 1999–2001. MMWR. 2003; 58:1065-1070. - PubMed
-
- Smith SC, Jr, Allen J, Blair SN, Bonow RO, Brass LM, Fonarow GC, Grundy SM, Hiratzka L, Jones D, Krumholz HM, Mosca L, Pearson T, Pfeffer MA, Taubert KA. AHA/ACC guidelines for secondary prevention for patients with coronary and other atherosclerotic vascular disease. J Am Coll Cardiol. 2006; 47:2130-2139. - PubMed
-
- Executive summary of the third report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III). JAMA. 2001; 285:2486-2497. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
