

Safety and Tumor Specificity of Cetuximab-IRDye800 for Surgical Navigation in Head and Neck Cancer
- PMID: 25904751
- PMCID: PMC4909371
- DOI: 10.1158/1078-0432.CCR-14-3284
Safety and Tumor Specificity of Cetuximab-IRDye800 for Surgical Navigation in Head and Neck Cancer
Abstract
Purpose: Positive margins dominate clinical outcomes after surgical resections in most solid cancer types, including head and neck squamous cell carcinoma. Unfortunately, surgeons remove cancer in the same manner they have for a century with complete dependence on subjective tissue changes to identify cancer in the operating room. To effect change, we hypothesize that EGFR can be targeted for safe and specific real-time localization of cancer.
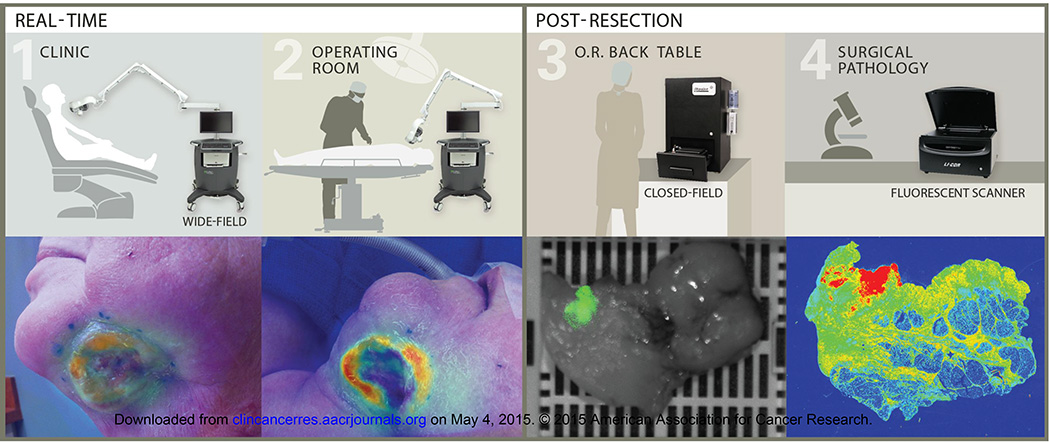
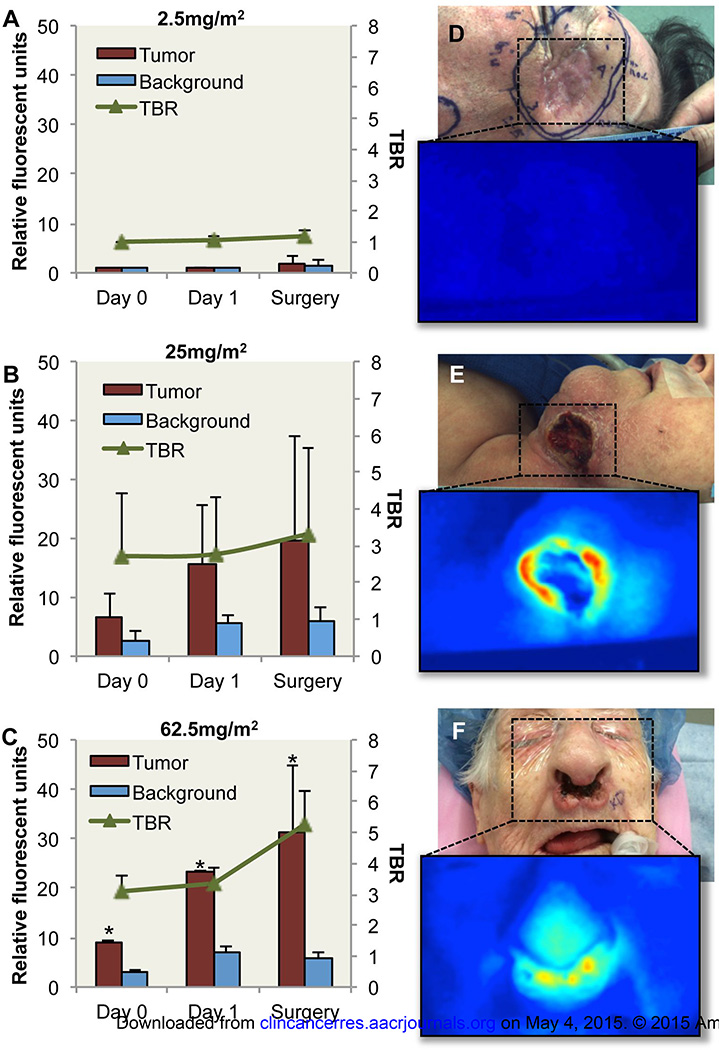
Experimental design: A dose escalation study of cetuximab conjugated to IRDye800 was performed in patients (n = 12) undergoing surgical resection of squamous cell carcinoma arising in the head and neck. Safety and pharmacokinetic data were obtained out to 30 days after infusion. Multi-instrument fluorescence imaging was performed in the operating room and in surgical pathology.
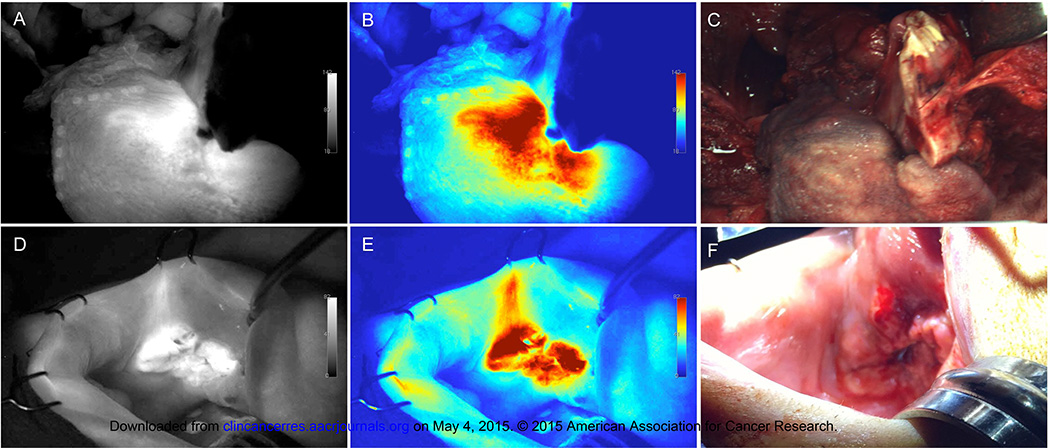
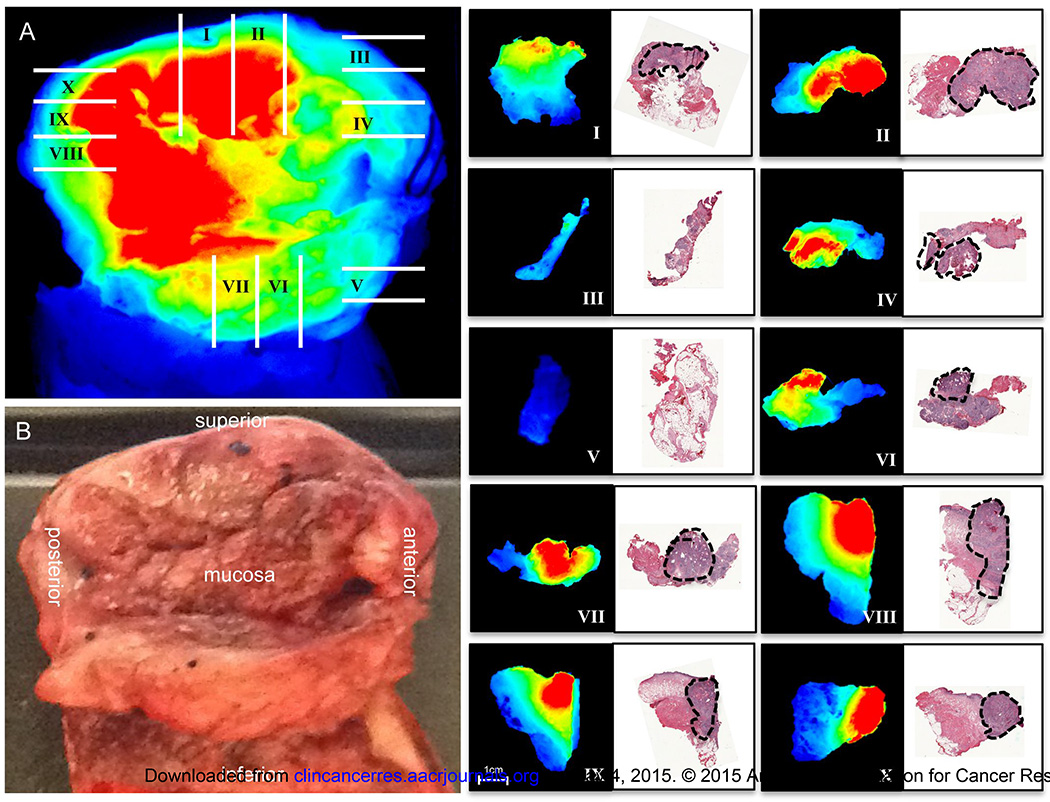
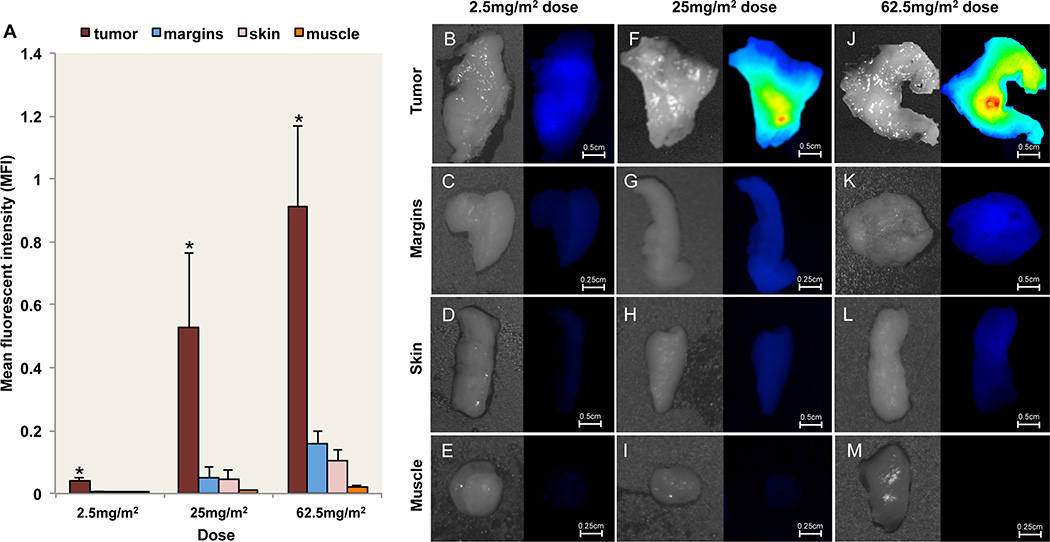
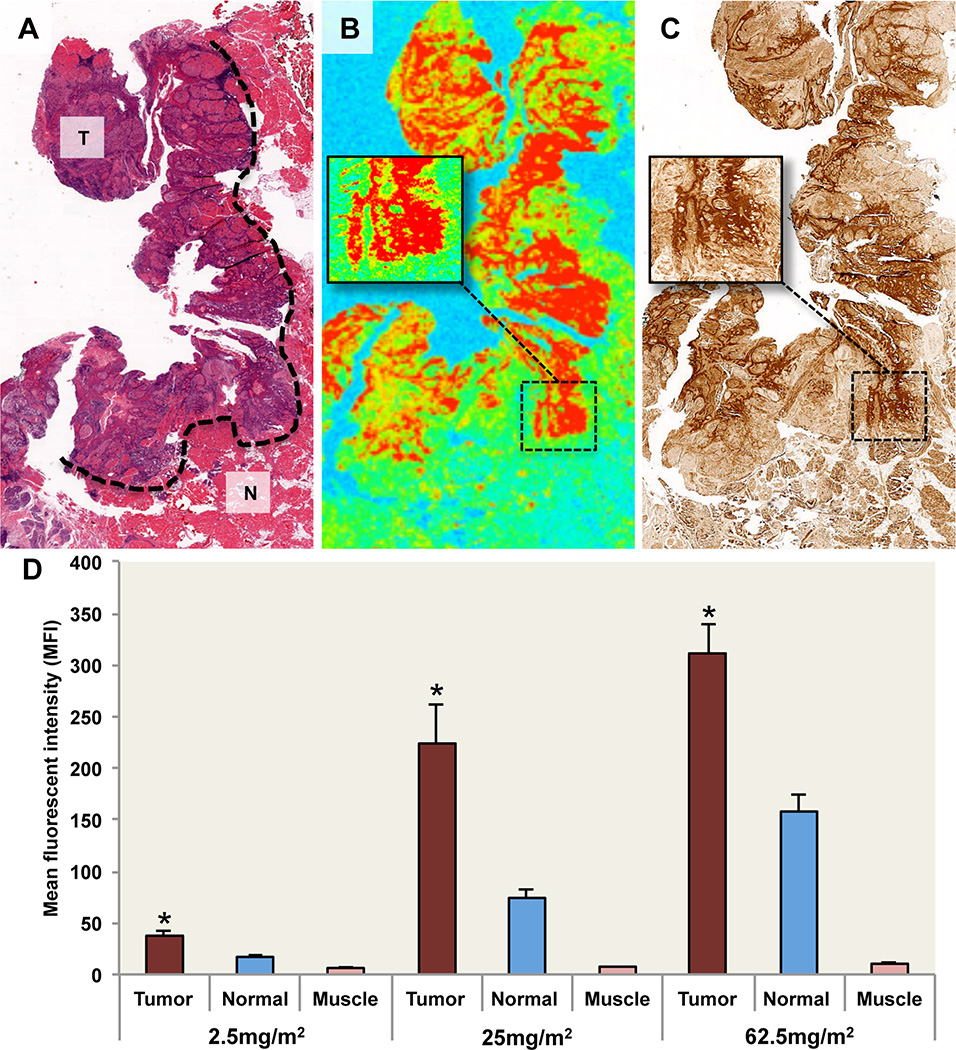
Results: There were no grade 2 or higher adverse events attributable to cetuximab-IRDye800. Fluorescence imaging with an intraoperative, wide-field device successfully differentiated tumor from normal tissue during resection with an average tumor-to-background ratio of 5.2 in the highest dose range. Optical imaging identified opportunity for more precise identification of tumor during the surgical procedure and during the pathologic analysis of tissues ex vivo. Fluorescence levels positively correlated with EGFR levels.
Conclusions: We demonstrate for the first time that commercially available antibodies can be fluorescently labeled and safely administered to humans to identify cancer with sub-millimeter resolution, which has the potential to improve outcomes in clinical oncology.
©2015 American Association for Cancer Research.
Conflict of interest statement
The authors report no conflict of interest.
Figures
References
-
- Arbes SJ, Jr, Olshan AF, Caplan DJ, Schoenbach VJ, Slade GD, Symons MJ. Factors contributing to the poorer survival of black Americans diagnosed with oral cancer (United States) Cancer Causes Control. 1999;10:513–523. - PubMed
-
- Woolgar JA, Triantafyllou A. A histopathological appraisal of surgical margins in oral and oropharyngeal cancer resection specimens. Oral Oncol. 2005 - PubMed
-
- McMahon J, O'Brien CJ, Pathak I, Hamill R, McNeil E, Hammersley N, et al. Influence of condition of surgical margins on local recurrence and disease-specific survival in oral and oropharyngeal cancer. Br J Oral Maxillofac Surg. 2003;41:224–231. - PubMed
-
- Hinni ML, Ferlito A, Brandwein-Gensler MS, Takes RP, Silver CE, Westra WH, et al. Surgical margins in head and neck cancer: a contemporary review. Head Neck. 2013;35:1362–1370. - PubMed
-
- Stummer W, Pichlmeier U, Meinel T, Wiestler OD, Zanella F, Reulen HJ, et al. Fluorescence-guided surgery with 5-aminolevulinic acid for resection of malignant glioma: a randomised controlled multicentre phase III trial. The lancet oncology. 2006;7:392–401. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
