

An Analysis of Cesarean Section and Emergency Hernia Ratios as Markers of Surgical Capacity in Low-Income Countries Affected by Humanitarian Emergencies from 2008 - 2014 at Médecins sans Frontières Operations Centre Brussels Projects
- PMID: 25905025
- PMCID: PMC4395259
- DOI: 10.1371/currents.dis.5e30807568eaad09a3e23282ddb41da6
An Analysis of Cesarean Section and Emergency Hernia Ratios as Markers of Surgical Capacity in Low-Income Countries Affected by Humanitarian Emergencies from 2008 - 2014 at Médecins sans Frontières Operations Centre Brussels Projects
Abstract
Background: Surgical capacity assessments in low-income countries have demonstrated critical deficiencies. Though vital for planning capacity improvements, these assessments are resource intensive and impractical during the planning phase of a humanitarian crisis. This study aimed to determine cesarean sections to total operations performed (CSR) and emergency herniorrhaphies to all herniorrhaphies performed (EHR) ratios from Médecins Sans Frontières Operations Centre Brussels (MSF-OCB) projects and examine if these established metrics are useful proxies for surgical capacity in low-income countries affected by crisis.
Methods: All procedures performed in MSF-OCB operating theatres from July 2008 through June 2014 were reviewed. Projects providing only specialty care, not fully operational or not offering elective surgeries were excluded. Annual CSRs and EHRs were calculated for each project. Their relationship was assessed with linear regression.
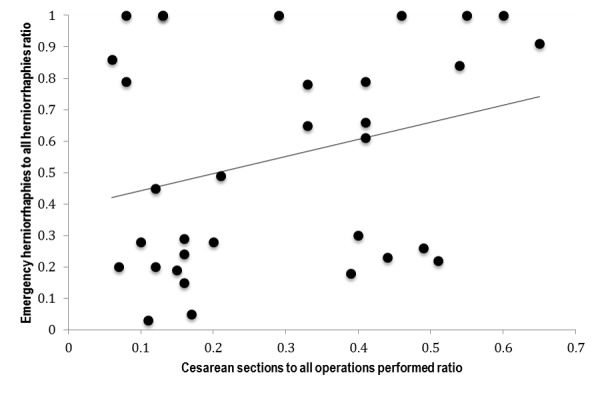
Results: After applying the exclusion criteria, there were 47,472 cases performed at 13 sites in 8 countries. There were 13,939 CS performed (29% of total cases). Of the 4,632 herniorrhaphies performed (10% of total cases), 30% were emergency procedures. CSRs ranged from 0.06 to 0.65 and EHRs ranged from 0.03 to 1.0. Linear regression of annual ratios at each project did not demonstrate statistical evidence for the CSR to predict EHR [F(2,30)=2.34, p=0.11, R2=0.11]. The regression equation was: EHR = 0.25 + 0.52(CSR) + 0.10(reason for MSF-OCB assistance).
Conclusion: Surgical humanitarian assistance projects operate in areas with critical surgical capacity deficiencies that are further disrupted by crisis. Rapid, accurate assessments of surgical capacity are necessary to plan cost- and clinically-effective humanitarian responses to baseline and acute unmet surgical needs in LICs affected by crisis. Though CSR and EHR may meet these criteria in 'steady-state' healthcare systems, they may not be useful during humanitarian emergencies. Further study of the relationship between direct surgical capacity improvements and these ratios is necessary to document their role in humanitarian settings.
Figures
References
-
- Stewart, B., et al., Global disease burden of conditions requiring emergency surgery. Br J Surg, 2014. 101(1): p. e9-22. - PubMed
-
- IHME. Data Visualizations. Global Burden of Disease Cause Patterns 2013 [cited 2014 12/7/2014]
-
- Groen, R.S., et al., Untreated surgical conditions in Sierra Leone: a cluster randomised, cross-sectional, countrywide survey. Lancet, 2012. 380(9847): p. 1082-7. - PubMed
-
- Gupta, S., et al., Surgical Needs of Nepal: Pilot Study of Population Based Survey in Pokhara, Nepal. World J Surg, 2014. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
