

Chemotherapy in glioma
- PMID: 25906059
- PMCID: PMC6088309
- DOI: 10.2217/cns.15.2
Chemotherapy in glioma
Abstract
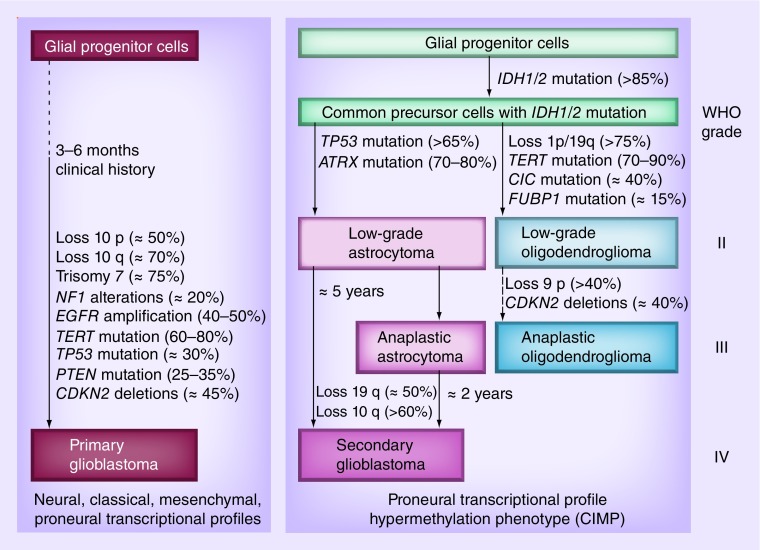
The treatment of glial brain tumors begins with surgery, and standard adjuvant treatment at the end of the past millennium for high-grade glioma and high-risk low-grade glioma was radiotherapy and chemotherapy was given at recurrence. However, over the past 10 years much has changed regarding the role of chemotherapy in gliomas and it is now clear that chemotherapy has a role in the treatment of almost all newly diagnosed diffuse gliomas (WHO grade II-IV). This is the result of several prospective studies that showed survival benefit after combined chemoradiotherapy with temozolomide in glioblastoma (WHO grade IV) or after procarbazine, CCNU (lomustine) and vincristine chemotherapy in diffuse low-grade (WHO grade II) and anaplastic (WHO grade III) glioma. The current standard of treatment for diffuse gliomas is described in this overview and in addition some attention is given to targeted therapies.
Keywords: anaplastic glioma; astrocytoma; chemotherapy; glioblastoma; glioma; high-grade glioma; low-grade glioma; oligoastrocytoma; oligodendroglioma.
Conflict of interest statement
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous