

Cluster Analysis in Patients with GOLD 1 Chronic Obstructive Pulmonary Disease
- PMID: 25906326
- PMCID: PMC4407903
- DOI: 10.1371/journal.pone.0123626
Cluster Analysis in Patients with GOLD 1 Chronic Obstructive Pulmonary Disease
Abstract
Background: We hypothesized that heterogeneity exists within the Global Initiative for Chronic Obstructive Lung Disease (GOLD) 1 spirometric category and that different subgroups could be identified within this GOLD category.
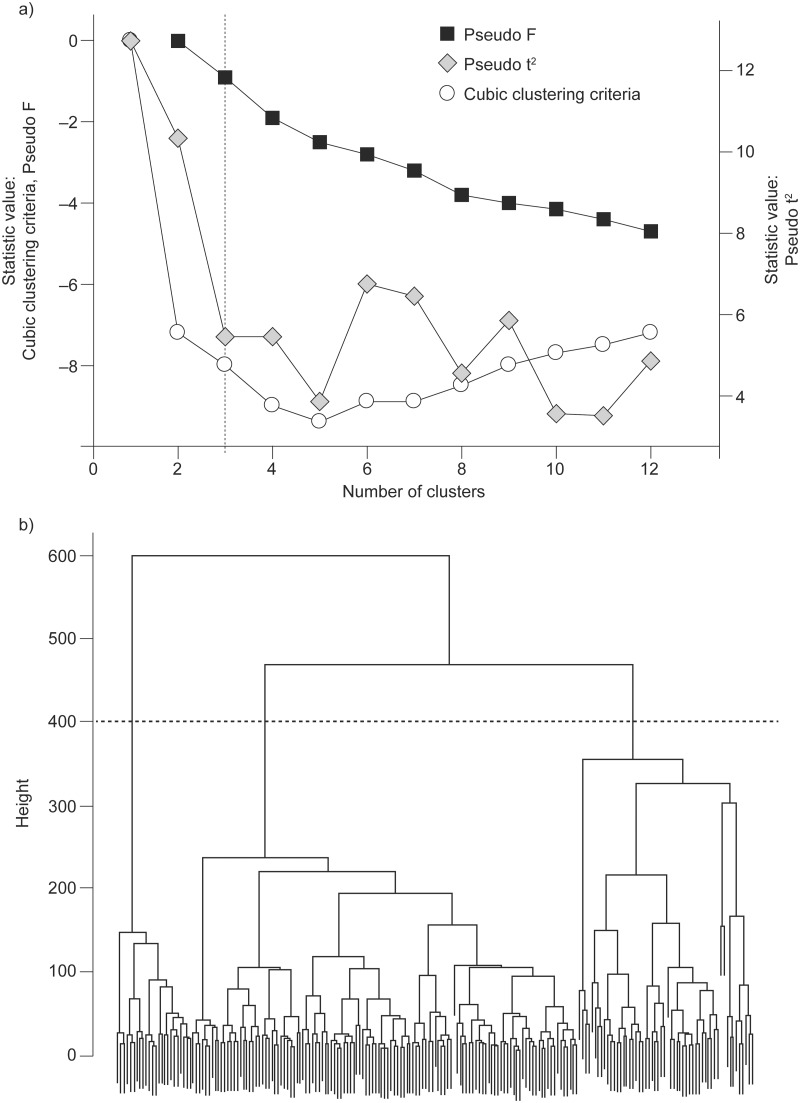
Methods: Pre-randomization study participants from two clinical trials were symptomatic/asymptomatic GOLD 1 chronic obstructive pulmonary disease (COPD) patients and healthy controls. A hierarchical cluster analysis used pre-randomization demographics, symptom scores, lung function, peak exercise response and daily physical activity levels to derive population subgroups.
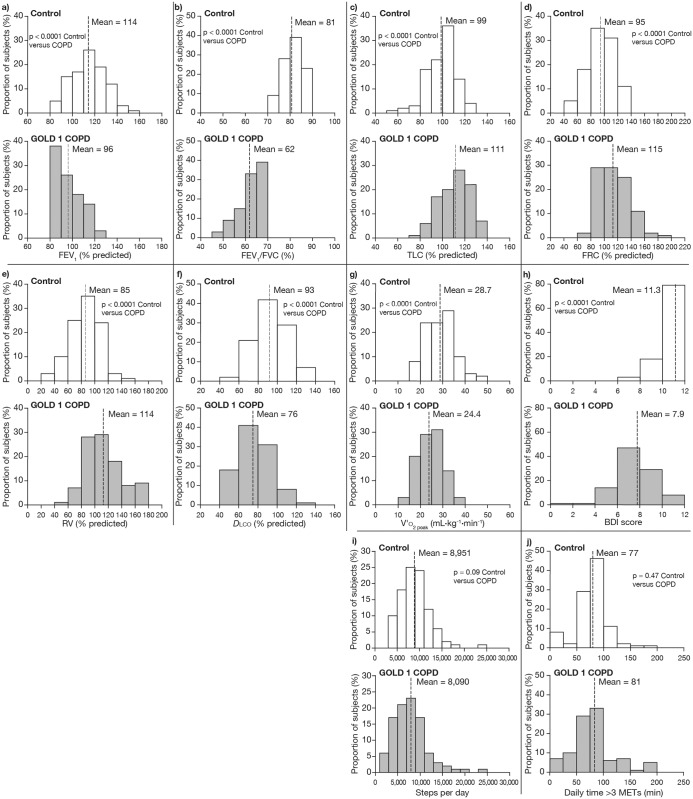
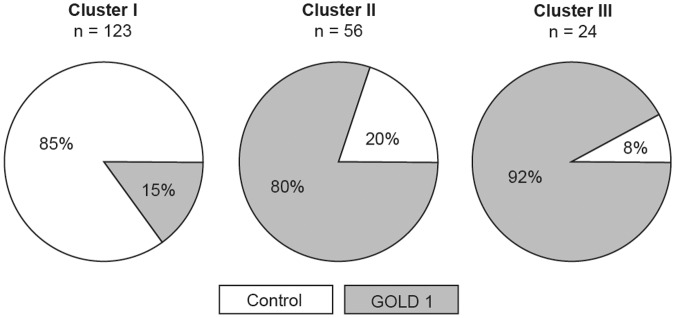
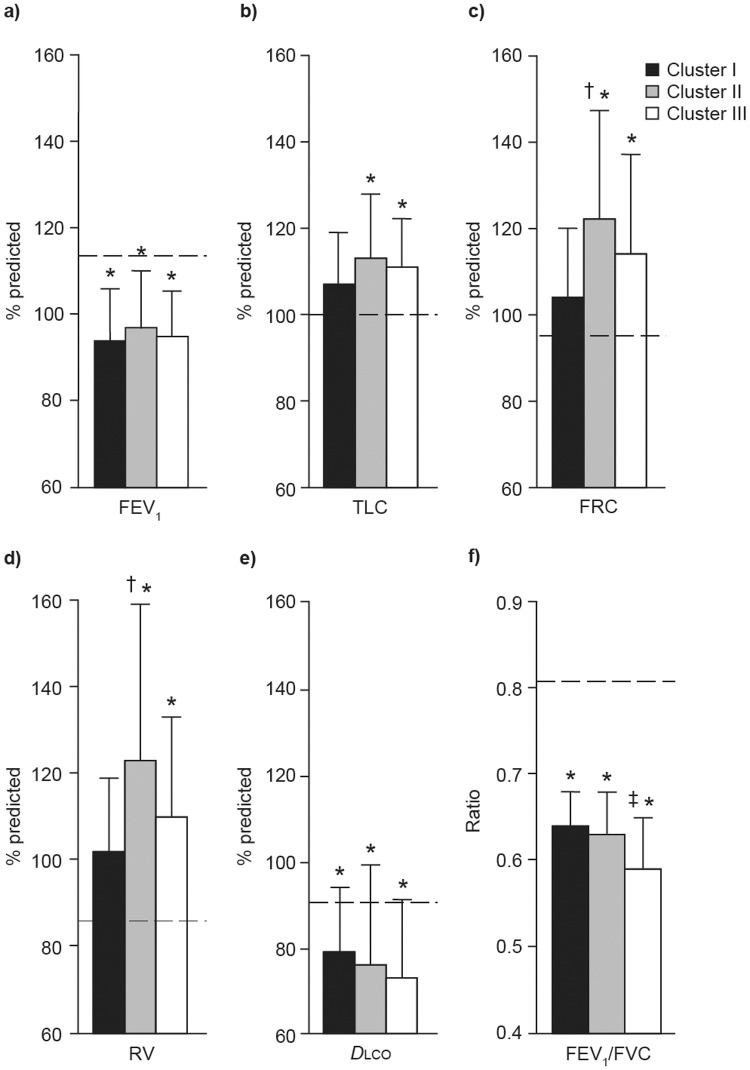
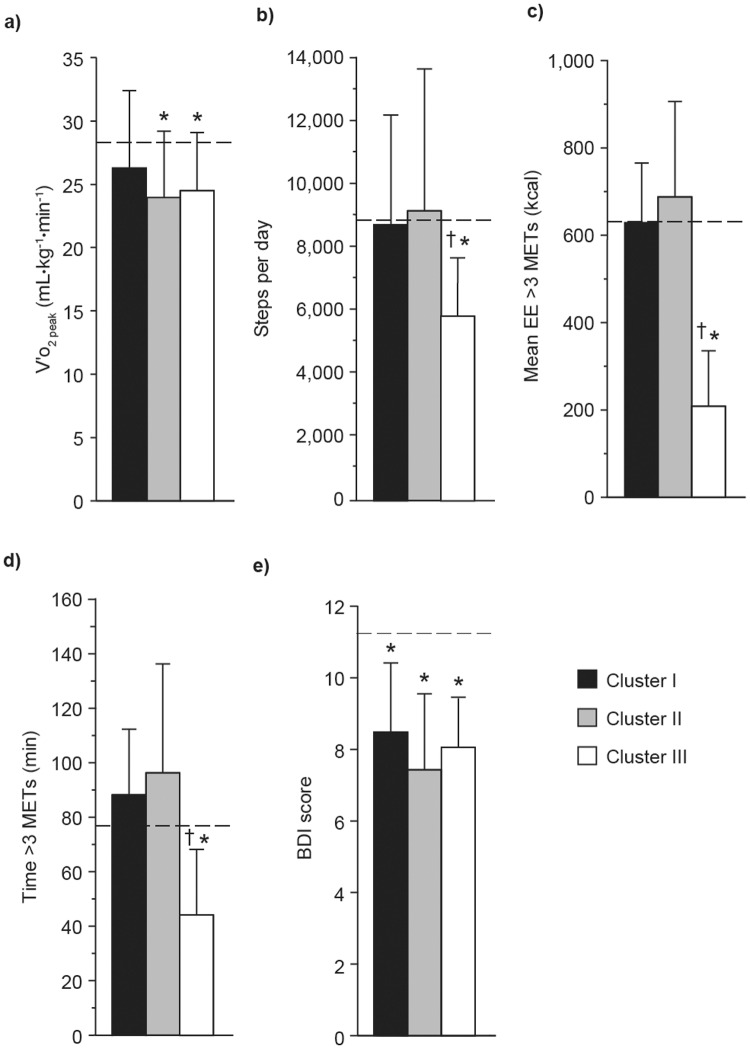
Results: Considerable heterogeneity existed for clinical variables among patients with GOLD 1 COPD. All parameters, except forced expiratory volume in 1 second (FEV1)/forced vital capacity (FVC), had considerable overlap between GOLD 1 COPD and controls. Three-clusters were identified: cluster I (18 [15%] COPD patients; 105 [85%] controls); cluster II (45 [80%] COPD patients; 11 [20%] controls); and cluster III (22 [92%] COPD patients; 2 [8%] controls). Apart from reduced diffusion capacity and lower baseline dyspnea index versus controls, cluster I COPD patients had otherwise preserved lung volumes, exercise capacity and physical activity levels. Cluster II COPD patients had a higher smoking history and greater hyperinflation versus cluster I COPD patients. Cluster III COPD patients had reduced physical activity versus controls and clusters I and II COPD patients, and lower FEV1/FVC versus clusters I and II COPD patients.
Conclusions: The results emphasize heterogeneity within GOLD 1 COPD, supporting an individualized therapeutic approach to patients.
Trial registration: www.clinicaltrials.gov. NCT01360788 and NCT01072396.
Conflict of interest statement
Figures
References
-
- Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. January 2014. Available: http://www.goldcopd.org/uploads/users/files/GOLD_Report_2014_Jan23.pdf. Accessed 29 April 2014.
-
- Buist AS, McBurnie MA, Vollmer WM, Gillespie S, Burney P, Mannino DM, et al. International variation in the prevalence of COPD (the BOLD Study): a population-based prevalence study. Lancet. 2007;370: 741–750. - PubMed
-
- Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. November 2006. Available: http://www.goldcopd.org/uploads/users/files/GOLDReport2006_0122.pdf. Accessed 29 April 2014.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
