

Feasibility and Reproducibility of Echocardiographic Measures in Children with Muscular Dystrophies
- PMID: 25906753
- PMCID: PMC4526320
- DOI: 10.1016/j.echo.2015.03.003
Feasibility and Reproducibility of Echocardiographic Measures in Children with Muscular Dystrophies
Abstract
Background: Cardiac disease is a major cause of death in patients with muscular dystrophies. The use of feasible and reproducible echocardiographic measures of cardiac function is critical to advance the field of therapeutics for dystrophic cardiomyopathy.
Methods: Participants aged 8 to 18 years with genetically confirmed Duchenne muscular dystrophy (DMD), Becker muscular dystrophy, or limb-girdle muscular dystrophy were enrolled at five centers, and standardized echocardiographic examinations were performed. Measures of systolic and diastolic function and speckle-tracking echocardiography-derived cardiac strain were reviewed independently by two central readers. Furthermore, echocardiographic measures from participants with DMD were compared with those from retrospective age-matched control subjects from a single site to assess measures of myocardial function.
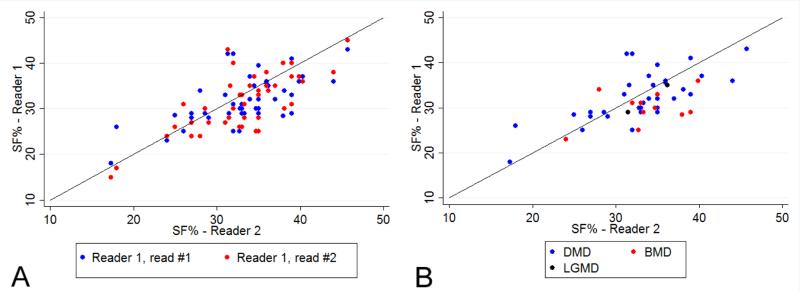
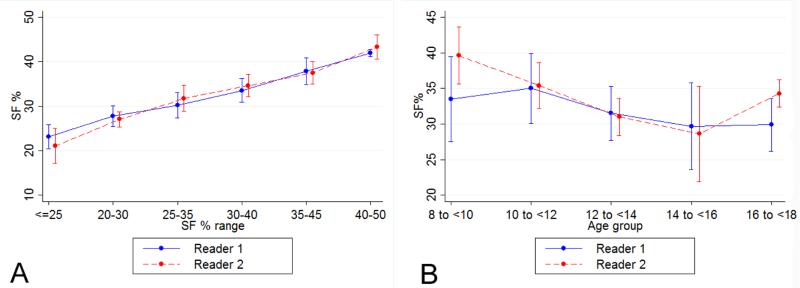
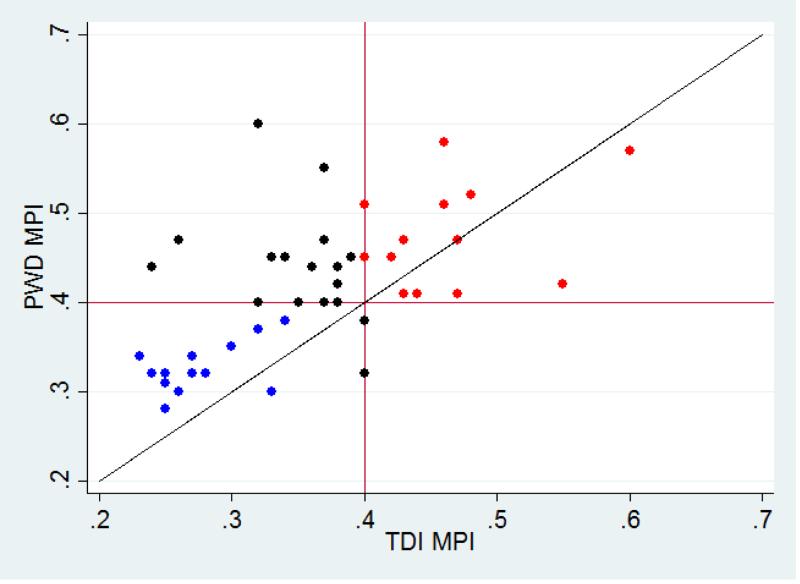
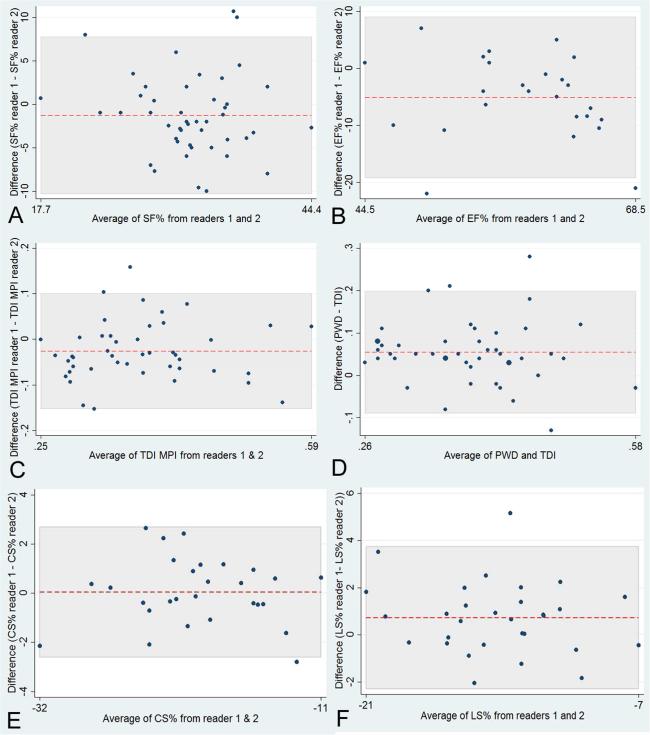
Results: Forty-eight participants (mean age, 13.3 ± 2.7 years) were enrolled. Shortening fraction had a greater interobserver correlation (intraclass correlation coefficient [ICC] = 0.63) compared with ejection fraction (ICC = 0.49). One reader could measure ejection fraction in only 53% of participants. Myocardial performance index measured by pulse-wave Doppler and Doppler tissue imaging showed similar ICCs (0.55 and 0.54). Speckle-tracking echocardiography showed a high ICC (0.96). Focusing on participants with DMD (n = 33), significantly increased mitral A-wave velocities, lower E/A ratios, and lower Doppler tissue imaging mitral lateral E' velocities were observed compared with age-matched control subjects. Speckle-tracking echocardiography demonstrated subclinical myocardial dysfunction with decreased average circumferential and longitudinal strain in three distinct subgroups: participants with DMD with normal shortening fractions, participants with DMD aged < 13 years, and participants with DMD with myocardial performance index scores < 0.40 compared with control subjects.
Conclusions: In a muscular dystrophy cohort, assessment of cardiac function is feasible and reproducible using shortening fraction, diastolic measures, and myocardial performance index. Cardiac strain measures identified early myocardial disease in patients with DMD.
Keywords: Cardiac strain; Cardiomyopathy; Echocardiography; Muscular dystrophy.
Copyright © 2015 American Society of Echocardiography. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Spurney CF. Cardiac Complications in Neuromuscular Disorders. In: Bertorini TE, editor. Neuromuscular Disorders: Treatment and Management. Elsevier; Philadelphia, PA: 2011. pp. 33–50.
-
- Nigro G, Comi LI, Politano L, Bain RJ. The incidence and evolution of cardiomyopathy in Duchenne muscular dystrophy. Int J Cardiol. 1990;26:271–7. - PubMed
-
- Spurney C, Shimizu R, Morgenroth LP, Kolski H, Gordish-Dressman H, Clemens PR. Cooperative international neuromuscular research group duchenne natural history study demonstrates insufficient diagnosis and treatment of cardiomyopathy in duchenne muscular dystrophy. Muscle Nerve. 2014;50:250–6. - PMC - PubMed
-
- Kajimoto H, Ishigaki K, Okumura K, Tomimatsu H, Nakazawa M, Saito K, et al. Beta-blocker therapy for cardiac dysfunction in patients with muscular dystrophy. Circ J. 2006;70:991–4. - PubMed
-
- Kirchmann C, Kececioglu D, Korinthenberg R, Dittrich S. Echocardiographic and electrocardiographic findings of cardiomyopathy in Duchenne and Becker-Kiener muscular dystrophies. Pediatr Cardiol. 2005;26:66–72. - PubMed
Publication types
MeSH terms
Grants and funding
- UL1 RR024153/RR/NCRR NIH HHS/United States
- UL1TR000002/TR/NCATS NIH HHS/United States
- 5ULRR024153-03/PHS HHS/United States
- UL1 TR000075/TR/NCATS NIH HHS/United States
- M01-RR00188/RR/NCRR NIH HHS/United States
- M01 RR000188/RR/NCRR NIH HHS/United States
- UL1RR024992/RR/NCRR NIH HHS/United States
- UL1 RR024992/RR/NCRR NIH HHS/United States
- 3UL1RR024153-04S5/RR/NCRR NIH HHS/United States
- UL1 TR000448/TR/NCATS NIH HHS/United States
- UL1 TR000002/TR/NCATS NIH HHS/United States
- UL1TR000075/TR/NCATS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
