

Restoring esophageal continuity following a failed colonic interposition for long-gap esophageal atresia
- PMID: 25907539
- PMCID: PMC4407410
- DOI: 10.1093/jscr/rjv048
Restoring esophageal continuity following a failed colonic interposition for long-gap esophageal atresia
Abstract
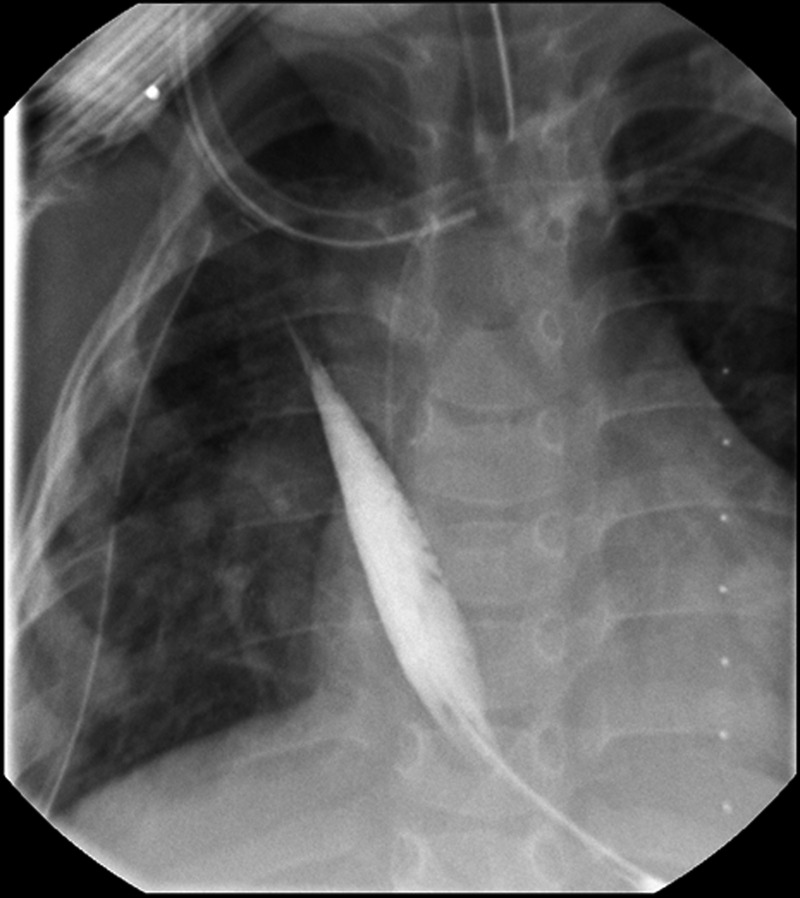
The Foker process is a method of esophageal lengthening through axial tension-induced growth, allowing for subsequent primary reconstruction of the esophagus in esophageal atresia (EA). In this unique case, the Foker process was used to grow the remaining esophageal segment long enough to attain esophageal continuity following failed colonic interpositions for long-gap esophageal atresia (LGEA). Initially developed for the treatment of LGEA in neonates, this case demonstrates that (i) an active esophageal lengthening response may still be present beyond the neonate time-period; and, (ii) the Foker process can be used to restore esophageal continuity following a failed colonic interposition if the lower esophageal segment is still present.
Published by Oxford University Press and JSCR Publishing Ltd. All rights reserved. © The Author 2015.
Figures



References
-
- Vogel A, Yang E, Fishman S. Hydrostatic stretch-induced growth facilitating primary anastomosis in long-gap esophageal atresia. J Pediatr Surg 2006;41:1170–2. - PubMed
-
- Domreis JS, Jobe BA, Aye RW, Deveney KE, Sheppard BC, Deveney CW. Management of long-term failure after colonic interposition for benign disease. Am J Surg 2002;183:544–6. - PubMed
-
- Gallo G, Zwaveling S, Groen H, Van der Zee D, Hulscher J. Long-gap esophageal atresia: a meta-analysis of jejunal interposition, colon interposition, and gastric pull-up. Eur J Pediatr Surg 2012;22:420–5. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
