

Left atrial enlargement and stroke recurrence: the Northern Manhattan Stroke Study
- PMID: 25908460
- PMCID: PMC4442058
- DOI: 10.1161/STROKEAHA.115.008711
Left atrial enlargement and stroke recurrence: the Northern Manhattan Stroke Study
Abstract
Background and purpose: Although left atrial enlargement (LAE) increases incident stroke risk, the association with recurrent stroke is less clear. Our aim was to determine the association of LAE with recurrent stroke most likely related to embolism (cryptogenic and cardioembolic) and all ischemic stroke recurrences.
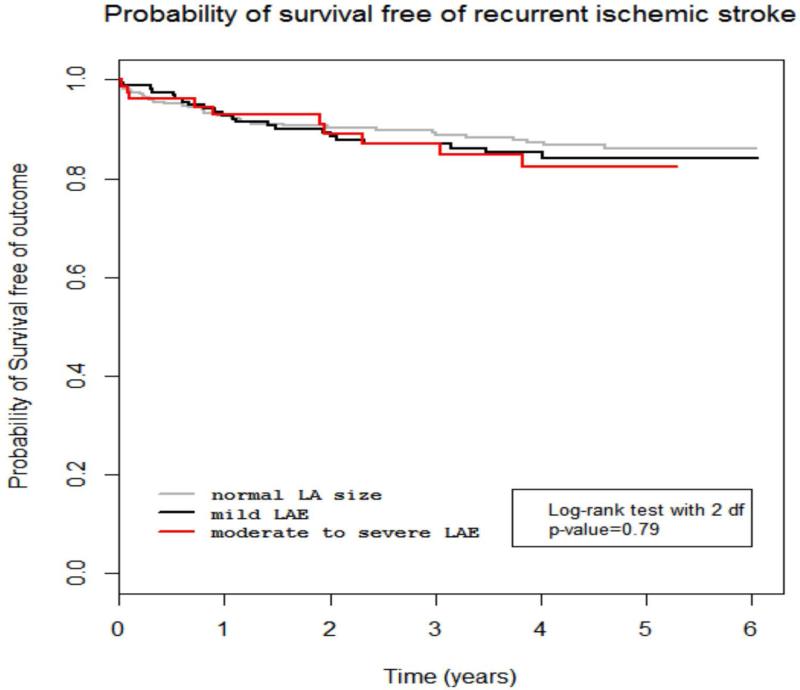
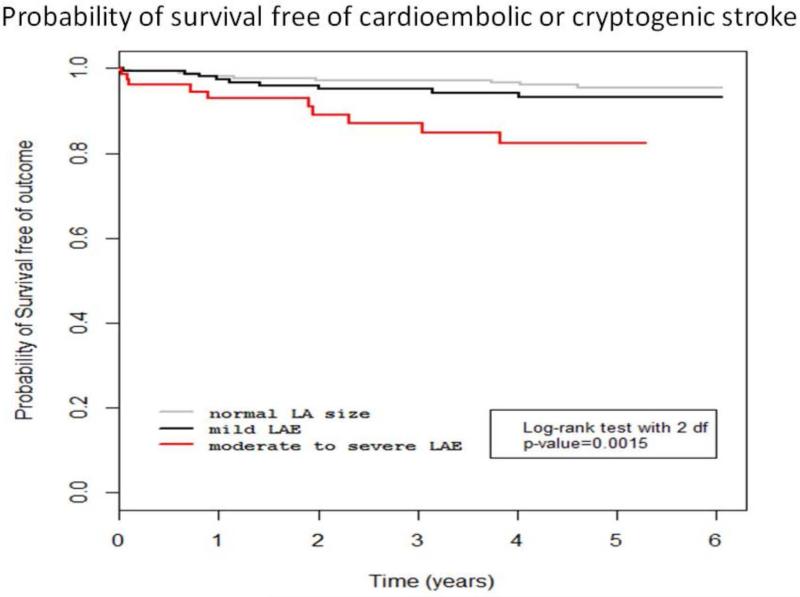
Methods: We followed 655 first ischemic stroke patients in the Northern Manhattan Stroke Study for ≤5 years. LA size from 2D echocardiography was categorized as normal LAE (52.7%), mild LAE (31.6%), and moderate-severe LAE (15.7%). We used Cox proportional hazard models to calculate the hazard ratios and 95% confidence intervals for the association of LA size and LAE with recurrent cryptogenic/cardioembolic and total recurrent ischemic stroke.
Results: LA size was available in 529 (81%) patients. Mean age at enrollment was 69±13 years; 45.8% were male, 54.0% Hispanic, and 18.5% had atrial fibrillation. Over a median of 4 years, there were 65 recurrent ischemic strokes (29 were cardioembolic or cryptogenic). In multivariable models adjusted for confounders, including atrial fibrillation and heart failure, moderate-severe LAE compared with normal LA size was associated with greater risk of recurrent cardioembolic/cryptogenic stroke (adjusted hazard ratio 2.83, 95% confidence interval 1.03-7.81), but not total ischemic stroke (adjusted hazard ratio 1.06, 95% confidence interval, 0.48-2.30). Mild LAE was not associated with recurrent stroke.
Conclusion: Moderate to severe LAE was an independent marker of recurrent cardioembolic or cryptogenic stroke in a multiethnic cohort of ischemic stroke patients. Further research is needed to determine whether anticoagulant use may reduce risk of recurrence in ischemic stroke patients with moderate to severe LAE.
Keywords: embolism.
© 2015 American Heart Association, Inc.
Figures
References
-
- Benjamin EJ, D'Agostino RB, Belanger AJ, Wolf PA, Levy D. Left atrial size and the risk of stroke and death. The framingham heart study. Circulation. 1995;92:835–841. - PubMed
-
- Di Tullio MR, Sacco RL, Sciacca RR, Homma S. Left atrial size and the risk of ischemic stroke in an ethnically mixed population. Stroke; a journal of cerebral circulation. 1999;30:2019–2024. - PubMed
-
- Wozakowska-Kaplon B. Changes in left atrial size in patients with persistent atrial fibrillation: A prospective echocardiographic study with a 5-year follow-up period. International journal of cardiology. 2005;101:47–52. - PubMed
-
- Mattioli AV, Sansoni S, Lucchi GR, Mattioli G. Serial evaluation of left atrial dimension after cardioversion for atrial fibrillation and relation to atrial function. The American journal of cardiology. 2000;85:832–836. - PubMed
