

Efficacy of Long-Term β-Blocker Therapy for Secondary Prevention of Long-Term Outcomes After Coronary Artery Bypass Grafting Surgery
- PMID: 25908770
- PMCID: PMC4472324
- DOI: 10.1161/CIRCULATIONAHA.114.014209
Efficacy of Long-Term β-Blocker Therapy for Secondary Prevention of Long-Term Outcomes After Coronary Artery Bypass Grafting Surgery
Abstract
Background: Conflicting results from recent observational studies have raised questions concerning the benefit of β-blockers for patients undergoing coronary artery bypass grafting (CABG). Furthermore, the efficacy of long-term β-blocker therapy in CABG patients after hospital discharge is uncertain.
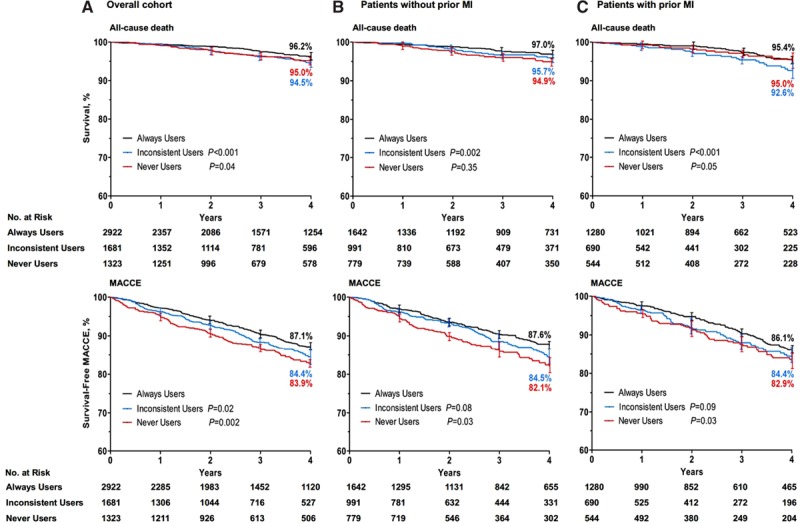
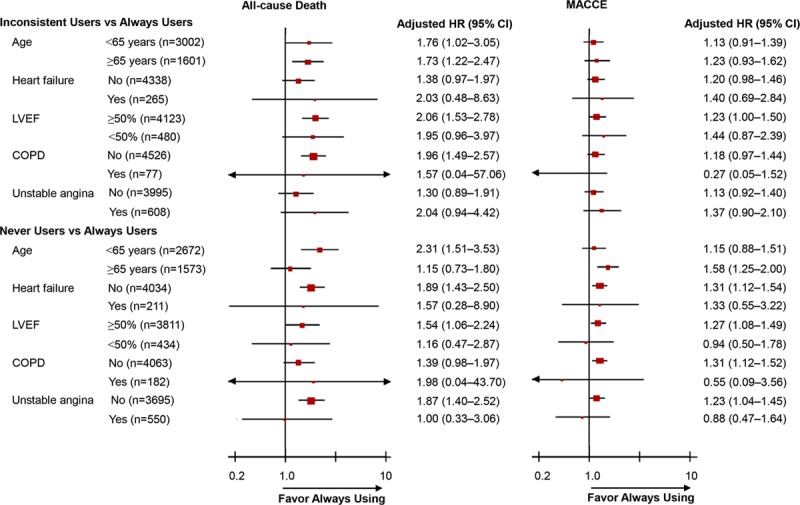
Methods and results: The study included 5926 consecutive patients who underwent CABG and were discharged alive. The prevalence and consistency of β-blocker use were determined in patients with and without a history of myocardial infarction (MI). β-Blockers were always used in 1280 patients (50.9%) with and 1642 patients (48.1%) without previous MI after CABG. Compared with always users (n=2922, 49.3%), the risk of all-cause death was significantly higher among inconsistent β-blocker users (hazard ratio [HR], 1.96; 95% confidence interval [CI], 1.50-2.57), and never using β-blockers was associated with increased risk of both all-cause death (HR, 1.42; 95% CI, 1.01-2.00) and the composite of adverse cardiovascular events (HR, 1.29; 95% CI, 1.10-1.50). In the cohort without MI, the HR for all-cause death was 1.70 (95% CI, 1.17-2.48) in inconsistent users and 1.23 (95% CI, 0.76-1.99) in never users. In the MI cohort, mortality was higher for inconsistent users (HR, 2.14; 95% CI, 1.43-3.20) and for never users (HR, 1.59; 95% CI, 1.07-2.63). Consistent results were obtained in equivalent sensitivity analyses.
Conclusions: In patients with or without previous MI undergoing CABG, the consistent use of β-blockers was associated with a lower risk of long-term mortality and adverse cardiovascular events. Strategies should be developed to understand and improve discharge prescription of β-blockers and long-term patient adherence.
Keywords: adrenergic beta-antagonists; coronary artery bypass; coronary artery disease; myocardial infarction.
© 2015 The Authors.
Figures
Comment in
-
Letter by Poullis Regarding Article, "Efficacy of Long-Term β-Blocker Therapy for Secondary Prevention of Long-Term Outcomes After Coronary Artery Bypass Grafting Surgery".Circulation. 2016 Feb 9;133(6):e391. doi: 10.1161/CIRCULATIONAHA.115.018190. Circulation. 2016. PMID: 26858297 No abstract available.
-
Letter by Bergerot et al Regarding Article, "Efficacy of Long-Term β-Blocker Therapy for Secondary Prevention of Long-Term Outcomes After Coronary Artery Bypass Grafting Surgery".Circulation. 2016 Feb 9;133(6):e392. doi: 10.1161/CIRCULATIONAHA.115.018316. Circulation. 2016. PMID: 26858298 No abstract available.
-
Letter by Kardesoglu et al Regarding Article, "Efficacy of Long-Term β-Blocker Therapy for Secondary Prevention of Long-Term Outcomes After Coronary Artery Bypass Grafting Surgery".Circulation. 2016 Feb 9;133(6):e393. doi: 10.1161/CIRCULATIONAHA.115.018675. Circulation. 2016. PMID: 26858299 No abstract available.
-
Response to Letters Regarding Article, "Efficacy of Long-Term β-Blocker Therapy for Secondary Prevention of Long-Term Outcomes After Coronary Artery Bypass Grafting Surgery".Circulation. 2016 Feb 9;133(6):e394-5. doi: 10.1161/CIRCULATIONAHA.115.019468. Circulation. 2016. PMID: 26858300 No abstract available.
References
-
- CAPRICORN Investigators. Effect of carvedilol on outcome after myocardial infarction in patients with left-ventricular dysfunction: the CAPRICORN randomised trial. Lancet. 2001;357:1385–1390. - PubMed
-
- Chen J, Radford MJ, Wang Y, Marciniak TA, Krumholz HM. Are beta-blockers effective in elderly patients who undergo coronary revascularization after acute myocardial infarction? Arch Intern Med. 2000;160:947–952. - PubMed
-
- Hillis LD, Smith PK, Anderson JL, Bittl JA, Bridges CR, Byrne JG, Cigarroa JE, Disesa VJ, Hiratzka LF, Hutter AM, Jr, Jessen ME, Keeley EC, Lahey SJ, Lange RA, London MJ, Mack MJ, Patel MR, Puskas JD, Sabik JF, Selnes O, Shahian DM, Trost JC, Winniford MD American College of Cardiology Foundation; American Heart Association Task Force on Practice Guidelines; American Association for Thoracic Surgery; Society of Cardiovascular Anesthesiologists; Society of Thoracic Surgeons. 2011 ACCF/AHA guideline for coronary artery bypass graft surgery: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines: developed in collaboration with the American Association for Thoracic Surgery, Society of Cardiovascular Anesthesiologists, and Society of Thoracic Surgeons. J Am Coll Cardiol. 2011;58:e123–e210. doi: 10.1016/j.jacc.2011.08.009. - PubMed
-
- Guru V, Anderson GM, Fremes SE, O’Connor GT, Grover FL, Tu JV Canadian CABG Surgery Quality Indicator Consensus Panel. The identification and development of Canadian coronary artery bypass graft surgery quality indicators. J Thorac Cardiovasc Surg. 2005;130:1257–1264. - PubMed
-
- Shahian DM, Edwards FH, Ferraris VA, Haan CK, Rich JB, Normand SL, DeLong ER, O’Brien SM, Shewan CM, Dokholyan RS, Peterson ED Society of Thoracic Surgeons Quality Measurement Task Force. Quality measurement in adult cardiac surgery, part 1: conceptual framework and measure selection. Ann Thorac Surg. 2007;83(suppl):S3–S12. doi: 10.1016/j.athoracsur.2007.01.053. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
