

Effects of epinephrine administration in out-of-hospital cardiac arrest based on a propensity analysis
- PMID: 25908979
- PMCID: PMC4407348
- DOI: 10.1186/2052-0492-1-12
Effects of epinephrine administration in out-of-hospital cardiac arrest based on a propensity analysis
Abstract
Background: Epinephrine administration has been advocated for cardiopulmonary resuscitation (CPR) for decades. Despite the fact that epinephrine administration during CPR is internationally accepted, the effects of the prehospital epinephrine administration still remain controversial. We investigated the effects of epinephrine administration on patients with out-of-hospital cardiac arrest based on a propensity analysis with regard to the 'CPR time'.
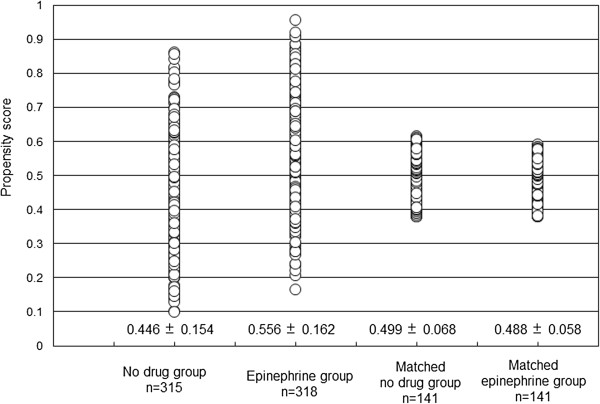
Methods: From April 1, 2007, to December 31, 2009, 633 out-of-hospital cardiac arrest patients with bystander witnesses were included in the present study. To rule out any survival bias, we used the propensity scores, which included CPR time. CPR time was defined as the time span from when the emergency medical technicians started CPR until either the return of spontaneous circulation or arrival at the hospital. After performing propensity score matching, the epinephrine and no-drug groups each included 141 patients. The primary study endpoint was a favorable neurological outcome at 30 days after cardiac arrest.
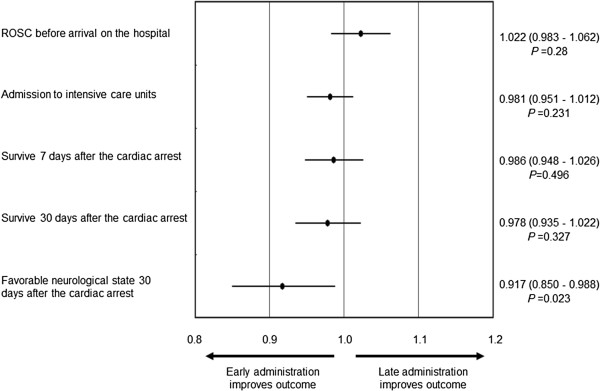
Results: After propensity score matching, the frequency of the return of spontaneous circulation before arrival at the hospital in the matched epinephrine group was higher than that in the matched no-drug group (27% vs. 13%, P = 0.002). However, the frequency of a favorable neurological state did not differ between the two groups. With regard to the frequency of a favorable neurological state in the patients, the adjusted odds ratio of the time span from cardiac arrest to the first epinephrine administration was 0.917 (95% confidence interval 0.850-0.988, P = 0.023) per minute.
Conclusions: In patients with witnessed out-of-hospital cardiac arrest, prehospital epinephrine administration was associated with increase of the return of spontaneous circulation before arrival at the hospital. Moreover, the early administration of epinephrine might improve the overall neurological outcome.
Keywords: Cardiac arrest; Epinephrine; Prehospital; Propensity analysis; Utstein.
Figures

References
-
- Hazinski MF, Nolan JP, Billi JE, Bottiger BW, Bossaert L, De Caen AR, Deakin CD, Drajer S, Eigel B, Hickey RW, Jacobs I, Kleinman ME, Kloeck W, Koster RW, Lim SH, Mancini ME, Montgomery WH, Morley PT, Morrison LJ, Nadkarni VM, O’Connor RE, Okada K, Perlman JM, Sayre MR, Shuster M, Soar J, Sunde K, Travers AH, Wyllie J, Zideman D. Part 1: executive summary: 2010 international consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations. Circulation. 2010;122(Suppl 2):250–275. doi: 10.1161/CIRCULATIONAHA.110.970897. - DOI - PubMed
-
- Stiell IG, Wells GA, Field B, Spaite DW, Nesbitt LP, De Maio VJ, Nichol G, Cousineau D, Blackburn J, Munkley D, Luinstra-Toohey L, Campeau T, Dagnone E, Lyver M. Advanced cardiac life support in out-of-hospital cardiac arrest. N Engl J Med. 2004;351:647–656. doi: 10.1056/NEJMoa040325. - DOI - PubMed
-
- Ohshige K, Shimazaki S, Hirasawa H, Nakamura M, Kin H, Fujii C, Okuchi K, Yamamoto Y, Akashi K, Takeda J, Hanyuda T, Tochikubo O. Evaluation of out-of-hospital cardiopulmonary resuscitation with resuscitative drugs: a prospective comparative study in Japan. Resuscitation. 2005;66:53–61. doi: 10.1016/j.resuscitation.2004.10.019. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
