

View-Angle Tilting and Slice-Encoding Metal Artifact Correction for Artifact Reduction in MRI: Experimental Sequence Optimization for Orthopaedic Tumor Endoprostheses and Clinical Application
- PMID: 25909472
- PMCID: PMC4409347
- DOI: 10.1371/journal.pone.0124922
View-Angle Tilting and Slice-Encoding Metal Artifact Correction for Artifact Reduction in MRI: Experimental Sequence Optimization for Orthopaedic Tumor Endoprostheses and Clinical Application
Abstract
Background: MRI plays a major role in follow-up of patients with malignant bone tumors. However, after limb salvage surgery, orthopaedic tumor endoprostheses might cause significant metal-induced susceptibility artifacts.
Purposes: To evaluate the benefit of view-angle tilting (VAT) and slice-encoding metal artifact correction (SEMAC) for MRI of large-sized orthopaedic tumor endoprostheses in an experimental model and to demonstrate clinical benefits for assessment of periprosthetic soft tissue abnormalities.
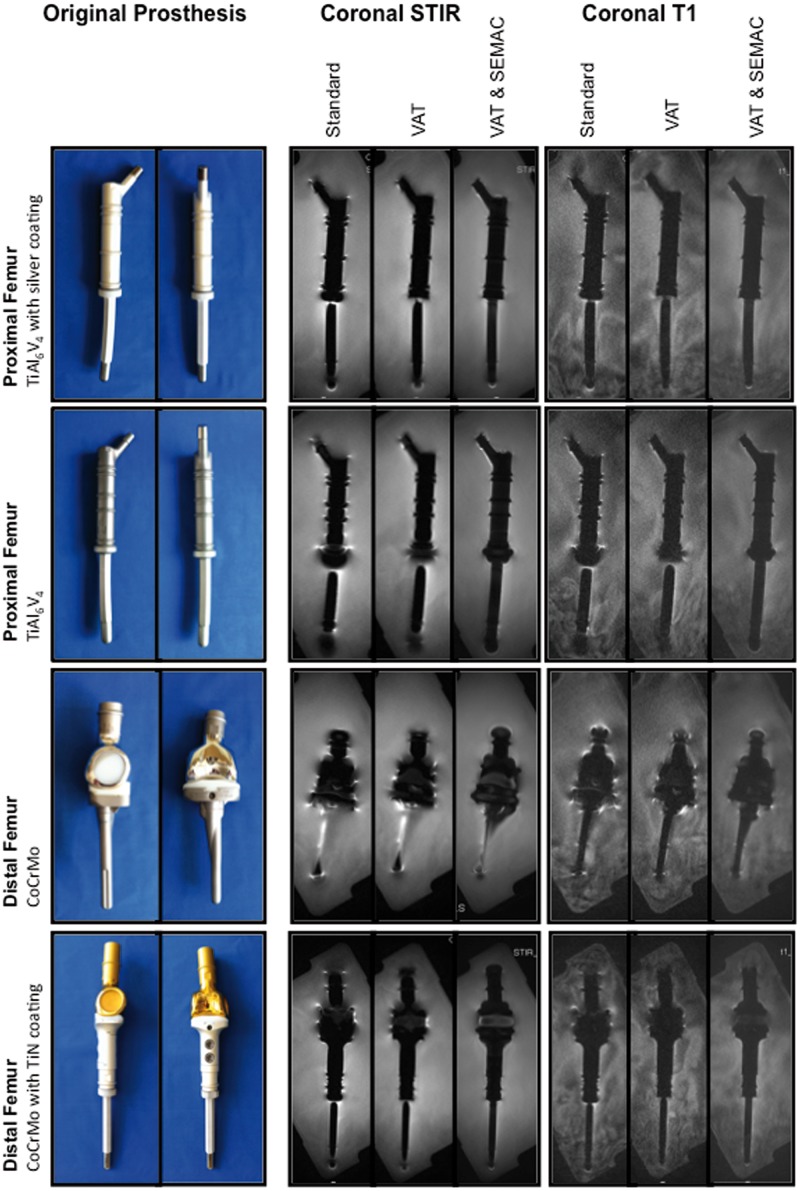
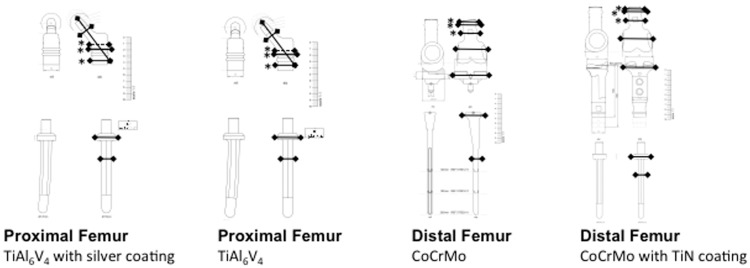
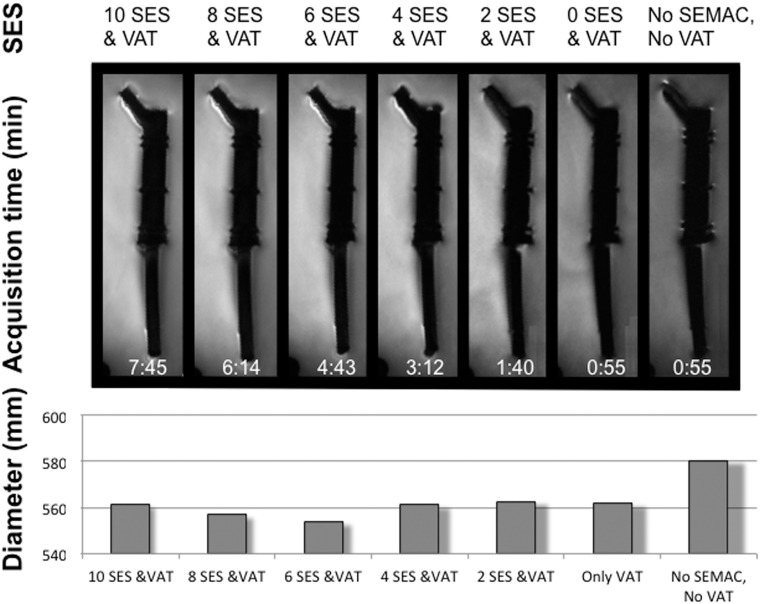
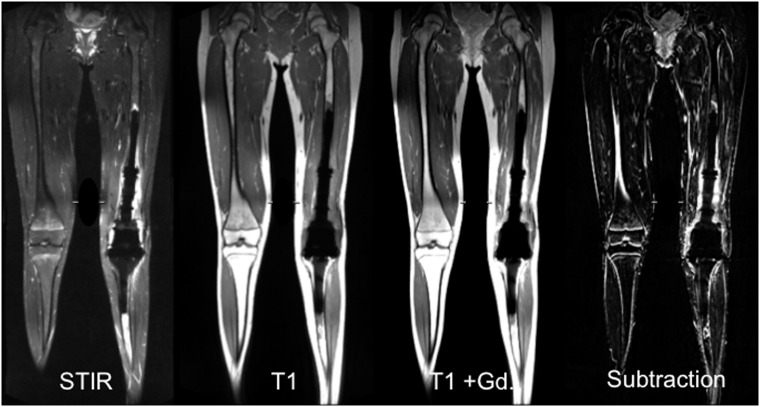
Methods: In an experimental setting, tumor endoprostheses (n=4) were scanned at 1.5T with three versions of optimized high-bandwidth turbo-spin-echo pulse sequences: (i) standard, (ii) VAT and (iii) combined VAT and SEMAC (VAT&SEMAC). Pulse sequences included coronal short-tau-inversion-recovery (STIR), coronal T1-weighted (w), transverse T1-w and T2-w TSE sequences. For clinical evaluation, VAT&SEMAC was compared to conventional metal artifact-reducing MR sequences (conventional MR) in n=25 patients with metal implants and clinical suspicion of tumor recurrence or infection. Diameters of artifacts were measured quantitatively. Qualitative parameters were assessed on a five-point scale (1=best, 5=worst): "image distortion", "artificial signal changes at the edges" and "diagnostic confidence". Imaging findings were correlated with pathology. T-tests and Wilcoxon-signed rank tests were used for statistical analyses.
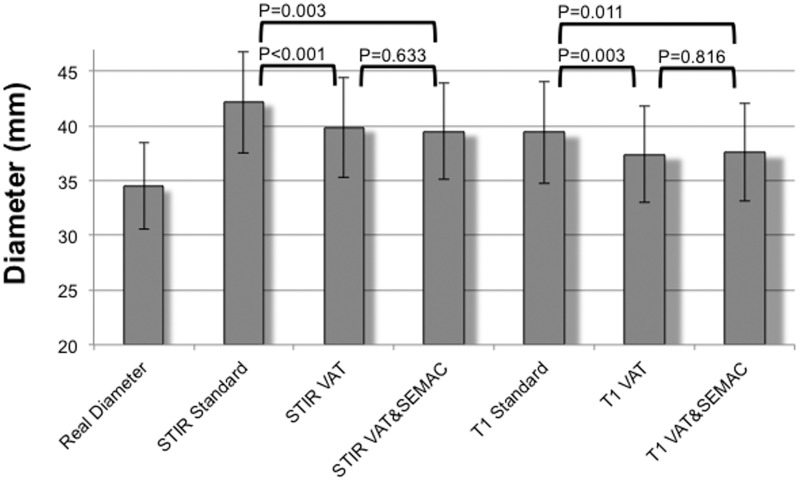
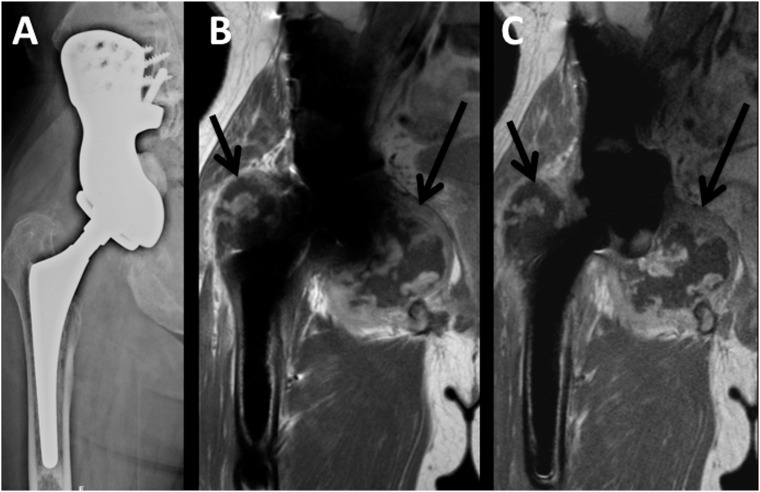
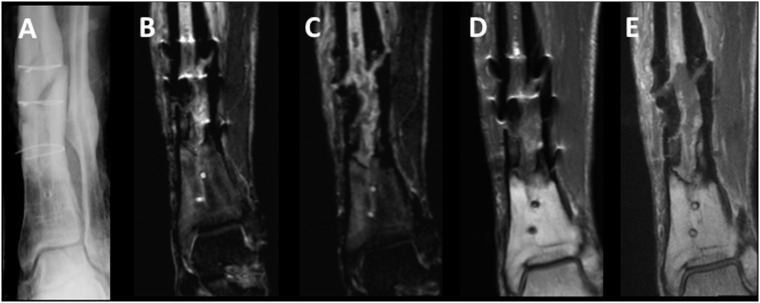
Results: The true size of the prostheses was overestimated on MRI (P<0.05). A significant reduction of artifacts was achieved by VAT (P<0.001) and VAT&SEMAC (P=0.003) compared to the standard group. Quantitative scores improved in the VAT and VAT&SEMAC group (P<0.05). On clinical MR images, artifact diameters were significantly reduced in the VAT&SEMAC-group as compared with the conventional-group (P<0.001). Distortion and artificial signal changes were reduced and diagnostic confidence improved (P<0.05). In two cases, tumor-recurrence, in ten cases infection and in thirteen cases other pathologies were diagnosed.
Conclusions: Significant reduction of metallic artifacts was achieved by VAT and SEMAC. Clinical results suggest, that these new techniques will be beneficial for detecting periprosthetic pathologies during postoperative follow-up.
Conflict of interest statement
Figures

References
-
- Choong PF, Sim FH, Pritchard DJ, Rock MG, Chao EY. Megaprostheses after resection of distal femoral tumors. A rotating hinge design in 30 patients followed for 2–7 years. Acta Orthop Scand. 1996;67(4):345–51. - PubMed
-
- Eckardt JJ, Eilber FR, Rosen G, Mirra JM, Dorey FJ, Ward WG, et al. Endoprosthetic replacement for stage IIB osteosarcoma. Clin Orthop Relat Res. 1991(270):202–13. - PubMed
-
- Kawai A, Muschler GF, Lane JM, Otis JC, Healey JH. Prosthetic knee replacement after resection of a malignant tumor of the distal part of the femur. Medium to long-term results. J Bone Joint Surg Am. 1998;80(5):636–47. - PubMed
-
- Morris HG, Capanna R, Campanacci D, Del Ben M, Gasbarrini A. Modular endoprosthetic replacement after total resection of the femur for malignant tumour. Int Orthop. 1994;18(2):90–5. - PubMed
-
- Sim FH, Frassica FJ, Chao EY. Orthopaedic management using new devices and prostheses. Clin Orthop Relat Res. 1995(312):160–72. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
