

Evidence and practice in spine registries
- PMID: 25909475
- PMCID: PMC4564774
- DOI: 10.3109/17453674.2015.1043174
Evidence and practice in spine registries
Abstract
Background and purpose: We performed a systematic review and a survey in order to (1) evaluate the evidence for the impact of spine registries on the quality of spine care, and with that, on patient-related outcomes, and (2) evaluate the methodology used to organize, analyze, and report the "quality of spine care" from spine registries.
Methods: To study the impact, the literature on all spinal disorders was searched. To study methodology, the search was restricted to degenerative spinal disorders. The risk of bias in the studies included was assessed with the Newcastle-Ottawa scale. Additionally, a survey among registry representatives was performed to acquire information about the methodology and practice of existing registries.
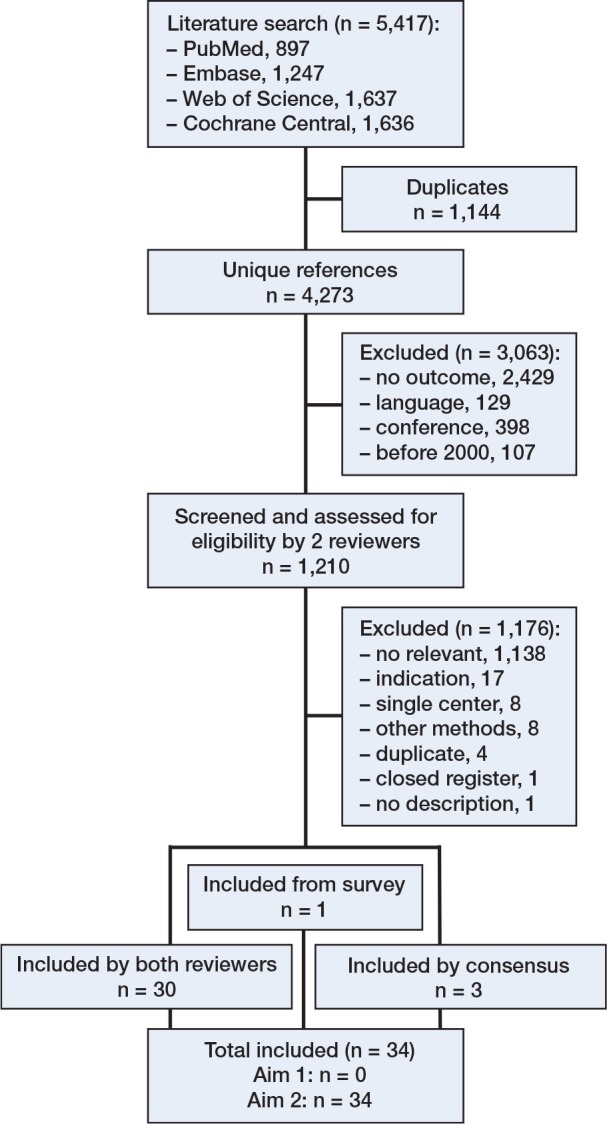
Results: 4,273 unique references up to May 2014 were identified, and 1,210 were eligible for screening and assessment. No studies on impact were identified, but 34 studies were identified to study the methodology. Half of these studies (17 of the 34) were judged to have a high risk of bias. The survey identified 25 spine registries, representing 14 countries. The organization of these registries, methods used, analytical approaches, and dissemination of results are presented.
Interpretation: We found a lack of evidence that registries have had an impact on the quality of spine care, regardless of whether intervention was non-surgical and/or surgical. To improve the quality of evidence published with registry data, we present several recommendations. Application of these recommendations could lead to registries showing trends, monitoring the quality of spine care given, and ultimately improving the value of the care given to patients with degenerative spinal disorders.
Figures
Comment in
-
Spinal disorders, quality-based healthcare and spinal registers.Acta Orthop. 2015;86(5):521-2. doi: 10.3109/17453674.2015.1072431. Epub 2015 Jul 13. Acta Orthop. 2015. PMID: 26169065 Free PMC article. No abstract available.
References
-
- Adogwa O, Huang M I, Thompson P M, et al. No difference in postoperative complications, pain, and functional outcomes up to 2 years after incidental durotomy in lumbar spinal fusion: a prospective, multi-institutional, propensity-matched analysis of 1,741 patients. Spine J. 2014;14(9):1828–34. - PubMed
-
- AHRQ. 2014. http://archive.ahrq.gov/consumer/qnt/qntqlook.html. 2015 Feb 09; Available. Accessed.
-
- Benson K, Hartz A J. A comparison of observational studies and randomized, controlled trials. N Engl J Med. 2000;342(25):1878–86. - PubMed
-
- Bridwell K H, Berven S, Glassman S, et al. Is the SRS-22 instrument responsive to change in adult scoliosis patients having primary spinal deformity surgery? Spine (Phila Pa 1976) 2007;32(20):2220–5. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical