

Dose-mass inverse optimization for minimally moving thoracic lesions
- PMID: 25909516
- PMCID: PMC4426070
- DOI: 10.1088/0031-9155/60/10/3927
Dose-mass inverse optimization for minimally moving thoracic lesions
Abstract
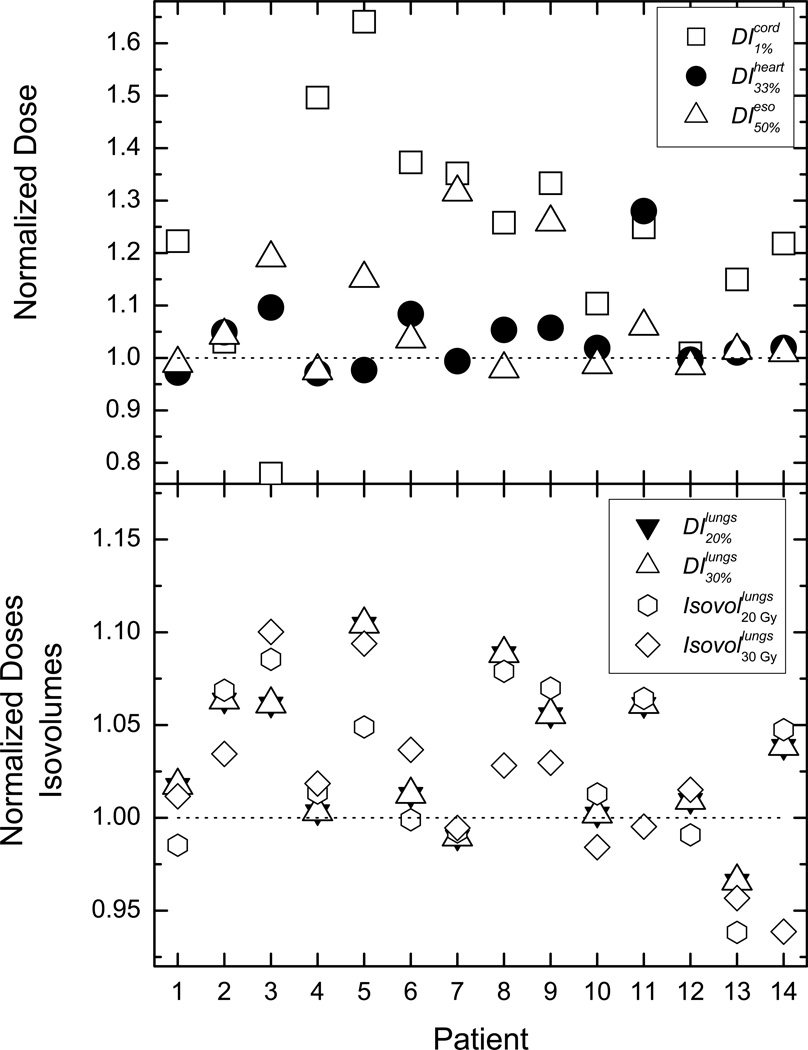
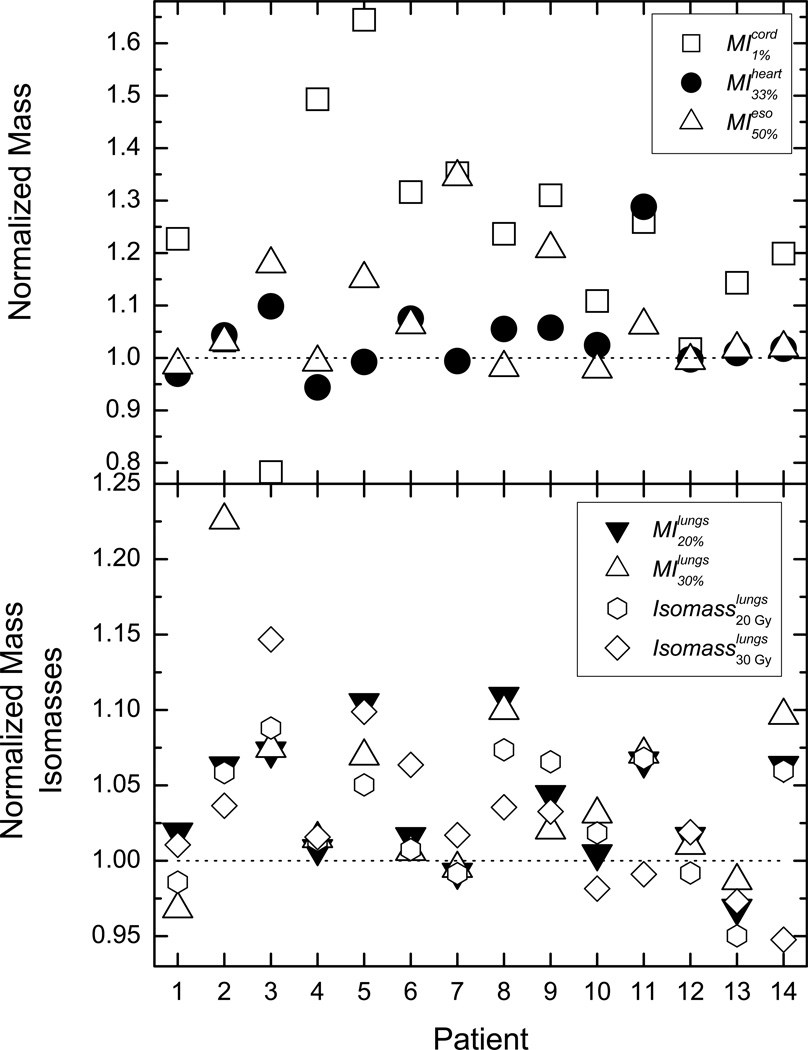
In the past decade, several different radiotherapy treatment plan evaluation and optimization schemes have been proposed as viable approaches, aiming for dose escalation or an increase of healthy tissue sparing. In particular, it has been argued that dose-mass plan evaluation and treatment plan optimization might be viable alternatives to the standard of care, which is realized through dose-volume evaluation and optimization. The purpose of this investigation is to apply dose-mass optimization to a cohort of lung cancer patients and compare the achievable healthy tissue sparing to that one achievable through dose-volume optimization. Fourteen non-small cell lung cancer (NSCLC) patient plans were studied retrospectively. The range of tumor motion was less than 0.5 cm and motion management in the treatment planning process was not considered. For each case, dose-volume (DV)-based and dose-mass (DM)-based optimization was performed. Nine-field step-and-shoot IMRT was used, with all of the optimization parameters kept the same between DV and DM optimizations. Commonly used dosimetric indices (DIs) such as dose to 1% the spinal cord volume, dose to 50% of the esophageal volume, and doses to 20 and 30% of healthy lung volumes were used for cross-comparison. Similarly, mass-based indices (MIs), such as doses to 20 and 30% of healthy lung masses, 1% of spinal cord mass, and 33% of heart mass, were also tallied. Statistical equivalence tests were performed to quantify the findings for the entire patient cohort. Both DV and DM plans for each case were normalized such that 95% of the planning target volume received the prescribed dose. DM optimization resulted in more organs at risk (OAR) sparing than DV optimization. The average sparing of cord, heart, and esophagus was 23, 4, and 6%, respectively. For the majority of the DIs, DM optimization resulted in lower lung doses. On average, the doses to 20 and 30% of healthy lung were lower by approximately 3 and 4%, whereas lung volumes receiving 2000 and 3000 cGy were lower by 3 and 2%, respectively. The behavior of MIs was very similar. The statistical analyses of the results again indicated better healthy anatomical structure sparing with DM optimization. The presented findings indicate that dose-mass-based optimization results in statistically significant OAR sparing as compared to dose-volume-based optimization for NSCLC. However, the sparing is case-dependent and it is not observed for all tallied dosimetric endpoints.
Figures
References
-
- Aaltonen P, Brahme A, Lax I, Levernes S, Naslund I, Reitan JB, Turesson I. Specification of dose delivery in radiation therapy. Recommendation by the Nordic Association of Clinical Physics (NACP) Acta oncologica (Stockholm, Sweden) 1997;36(Suppl 10):1–32. - PubMed
-
- American Cancer Society. Cancer Facts and Figures 2014. American Cancer Society. 2014
-
- Anscher MS, Marks LB, Shafman TD, Clough R, Huang H, Tisch A, Munley M, Herndon JE, Garst J, Crawford J, Jirtle RL. Risk of long-term complications after TFG-beta1-guided very-high-dose thoracic radiotherapy. International journal of radiation oncology, biology, physics. 2003;56:988–995. - PubMed
-
- Auperin A, Le Pechoux C, Pignon JP, Koning C, Jeremic B, Clamon G, Einhorn L, Ball D, Trovo MG, Groen HJ, Bonner JA, Le Chevalier T, Arriagada R. Concomitant radio-chemotherapy based on platin compounds in patients with locally advanced non-small cell lung cancer (NSCLC): a meta-analysis of individual data from 1764 patients. Ann oncol. 2006;17:473–483. - PubMed
-
- Belderbos J, Heemsbergen W, Hoogeman M, Pengel K, Rossi M, Lebesque J. Acute esophageal toxicity in non-small cell lung cancer patients after high dose conformal radiotherapy. Radiother oncol. 2005;75:157–164. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous