

Risk of gastrointestinal bleeding associated with oral anticoagulants: population based retrospective cohort study
- PMID: 25911526
- PMCID: PMC4413867
- DOI: 10.1136/bmj.h1585
Risk of gastrointestinal bleeding associated with oral anticoagulants: population based retrospective cohort study
Abstract
Objectives: To determine the real world safety of dabigatran or rivaroxaban compared with warfarin in terms of gastrointestinal bleeding.
Design: Retrospective cohort study.
Setting: Large administrative database of commercially insured people in United States from 1 October 2010 through 31 March 2012.
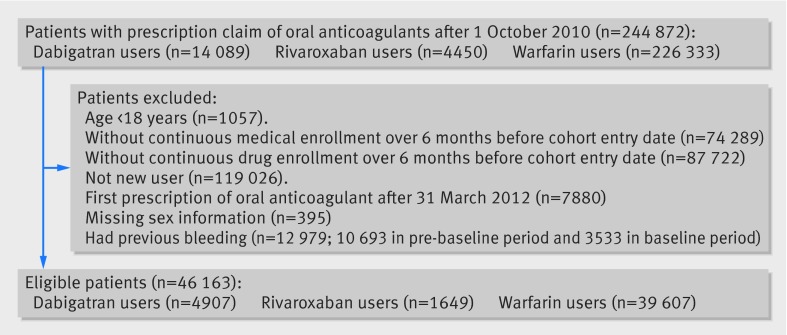
Participants: Enrollees with a prescription of warfarin, dabigatran, or rivaroxaban between 1 October 2010 and 31 March 2012, who were aged 18 years or older, had continuous enrollment and no oral anticoagulant use during the six months before the entry date, with known age and sex, and with no gastrointestinal bleeding for at least six months before the cohort entry date. The final study sample of 46,163 patients included 4907 using dabigatran, 1649 using rivaroxaban, and 39,607 using warfarin.
Main outcome measure: Time to gastrointestinal bleeding. Hazard ratios were derived from Cox proportional hazard models with propensity score weighting and robust estimates of errors.
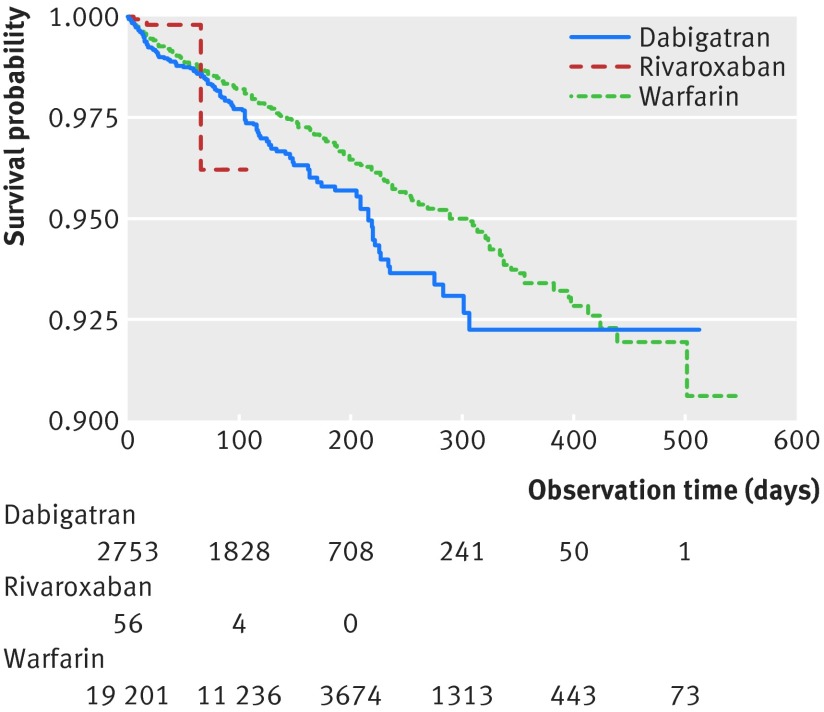
Results: Dabigatran users tended to be older (dabigatran v rivaroxaban v warfarin: 62.0 v 57.6 v 57.4 years) and more likely to be male (69% v 49% v 53%). The rate of gastrointestinal bleeding was highest among dabigatran users and lowest among rivaroxaban users (dabigatran v rivaroxaban v warfarin: 9.01 v 3.41 v 7.02 cases per 100 person years). After adjustment for potentially confounding covariates, there was no evidence of a statistically significant difference in the risk of gastrointestinal bleeding between dabigatran and warfarin users (adjusted hazard ratio 1.21, 95% confidence interval 0.96 to 1.53) or between rivaroxaban and warfarin users (0.98, 0.36 to 2.69).
Conclusions: Although rates of gastrointestinal bleeding seem to be similar in this commercially insured sample of adults in the United States, we cannot rule out as much as a 50% increase in the risk of gastrointestinal bleeding with dabigatran compared with warfarin or a more than twofold higher risk of bleeding with rivaroxaban compared with warfarin.
© Chang et al 2015.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
Comment in
-
Safety of new oral anticoagulants.BMJ. 2015 Apr 24;350:h1679. doi: 10.1136/bmj.h1679. BMJ. 2015. PMID: 25911527 No abstract available.
-
Anticoagulation therapy: Bleeding no worse with novel agents.Nat Rev Cardiol. 2015 Jul;12(7):381. doi: 10.1038/nrcardio.2015.75. Epub 2015 May 12. Nat Rev Cardiol. 2015. PMID: 25962977 No abstract available.
-
Meta-analysis should not be subject to selectivity and imbalance.BMJ. 2015 Jun 24;350:h3337. doi: 10.1136/bmj.h3337. BMJ. 2015. PMID: 26108537 No abstract available.
References
-
- Boehringer Ingelheim Pharmaceuticals. Pradaxa [package insert]. 2011.
-
- Janssen Pharmaceuticals. Xarelto [package insert]. 2011.
-
- Connolly SJ, Ezekowitz MD, Yusuf S, et al. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med 2009;361:1139-51. - PubMed
-
- Patel MR, Mahaffey KW, Garg J, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med 2011;365:883-91. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical