

Role for Surgical Resection in the Multidisciplinary Treatment of Stage IIIB Non-Small Cell Lung Cancer
- PMID: 25912748
- PMCID: PMC4562377
- DOI: 10.1016/j.athoracsur.2015.02.033
Role for Surgical Resection in the Multidisciplinary Treatment of Stage IIIB Non-Small Cell Lung Cancer
Abstract
Background: The role of multimodality therapy in stage IIIB non-small cell lung cancer (NSCLC) remains inadequately studied. Although chemoradiation is currently the mainstay of treatment, randomized trials evaluating surgical intervention are lacking, and resection is offered selectively.
Methods: Data from patients with clinical stage IIIB NSCLC (T4N2 or any N3) undergoing definitive multimodality therapy were obtained from the National Cancer Database (NCDB). Multivariable Cox regression models were fitted to evaluate variables influencing overall survival (OS).
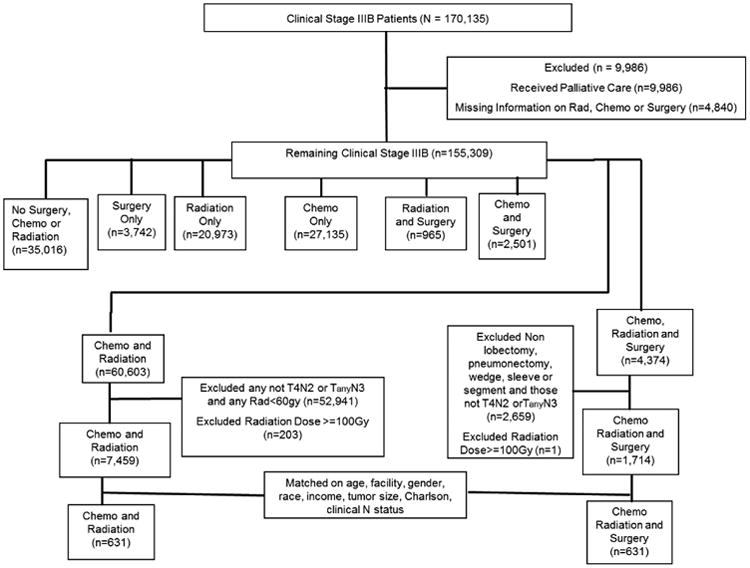
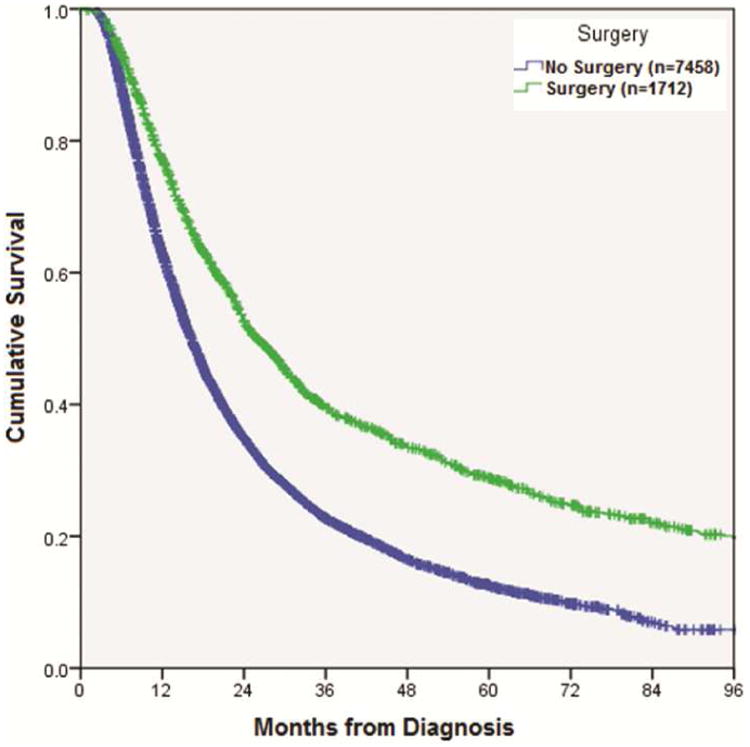
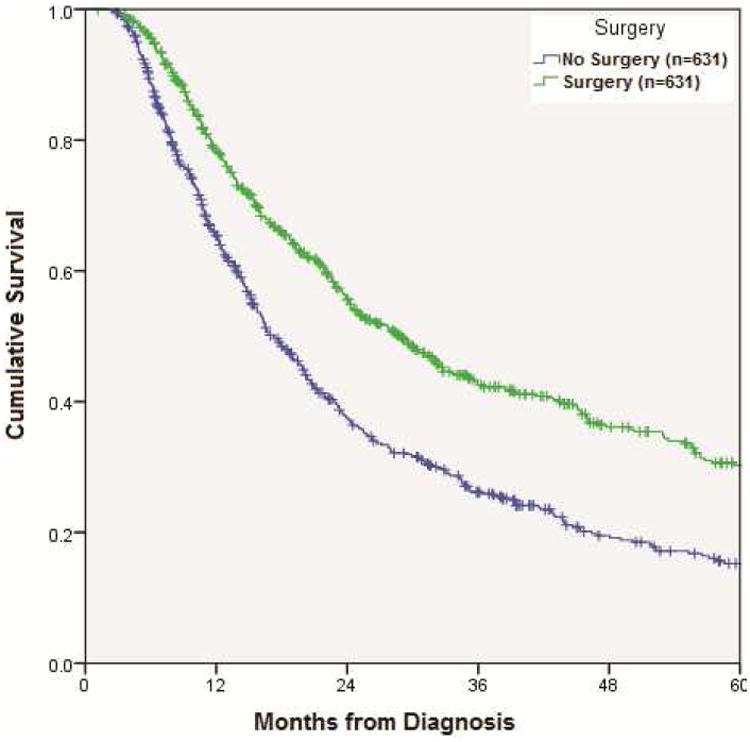
Results: From 1998 to 2010, 7,459 patients with clinical stage IIIB NSCLC were treated with definitive chemoradiation (CR group), whereas 1,714 patients underwent chemotherapy, radiation, and surgical intervention in any sequence (CRS group). CRS patients were more likely to be younger and white and have slightly smaller tumors (all p < 0.01). There was no difference in Charlson Comorbidity Index (CCI) between the groups (p = 0.5). In the CRS group, 79% of patients received neoadjuvant therapy. Thirty-day surgical mortality was 3%. Factors associated with improved OS in multivariate analysis included younger age, female sex, decreased CCI, smaller tumor size, and surgical resection (hazard ratio [HR], 0.57; 95% confidence interval [CI], 0.52-0.63). Among patients treated with surgical intervention, incomplete resection was associated with decreased OS (HR, 1.52; 95% CI, 1.20-1.92). Median OS was longer in the CRS group (25.9 months versus 16.3 months; p < 0.001). Propensity matched analysis on 631 patient pairs treated with CRS versus CR confirmed these findings (median OS, 28.9 versus 17.2 months; p < 0.001).
Conclusions: Surgical resection as a part of multimodality therapy may be associated with improved OS in highly selected patients with stage IIIB NSCLC. Multidisciplinary evaluation of these patients is critical.
Copyright © 2015 The Society of Thoracic Surgeons. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- American Cancer Society. Cancer Facts and Figures 2014. Atlanta: American Cancer Society; 2014.
-
- Edge SB, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A, editors. AJCC cancer staging manual. 7th. New York, NY: Springer; 2010.
-
- Ramnath N, Dilling TJ, Harris LJ, Kim AW, Michaud GC, Balekian AA, Diekemper R, Detterbeck FC, Arenberg DA. Treatment of Stage III Non-small Cell Lung Cancer - Diagnosis and Management of Lung Cancer, 3rd ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. CHEST. 2013;143(5 (Suppl)):e314S–e340S. - PubMed
-
- Goldstraw P, Crowley J, Chansky K, Giroux DJ, Groome PA, Rami-Porta R, Postmus PE, Rusch V, Sobin L. The IASLC Lung Cancer Staging Project: Proposals for the Revision of the TNM Stage Groupings in the Forthcoming (Seventh) Edition of the TNM Classification of Malignant Tumours. J Thorac Oncol. 2007;2:706–714. - PubMed
-
- Albain KS, Rusch VW, Crowley JJ, Rice TW, Turrisi AT, Weick JK, Lonchyna VA, Presant CA, McKenna RJ, Gandara DR, Fosmire H, Taylor SA, Stelzer KJ, Beasley KR, Livingston RB. Concurrent Cisplatin/Etoposide Plus Chest Radiotherapy Followed by Surgery for Stages IIIA (N2) and IIIB Non-Small-Cell Lung Cancer: Mature Results of Southwest Oncology Group Phase II Study 8805. J Clin Oncol. 1995;13:1880–1892. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
