

Screening Performance and Costs of Different Strategies in Prenatal Screening for Trisomy 21
- PMID: 25914417
- PMCID: PMC4397935
- DOI: 10.1055/s-0035-1545885
Screening Performance and Costs of Different Strategies in Prenatal Screening for Trisomy 21
Abstract
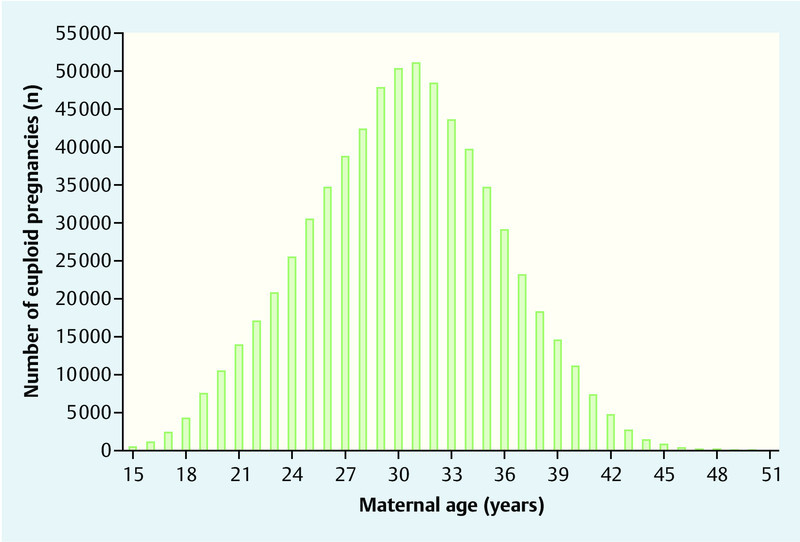
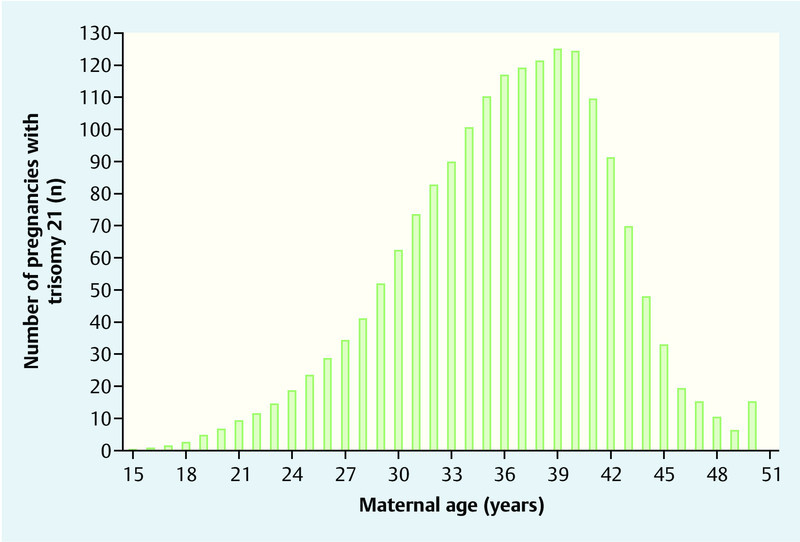
Objective: Cell-free fetal DNA (cffDNA) testing has opened new options in prenatal screening for trisomy 21. Due to the higher costs of cffDNA testing there is an ongoing debate on how to combine different screening strategies. Methods: For this study, a model-based approach was used to evaluate all births in Germany in 2012 together with the percentage of euploid and trisomic pregnancies. Detection rates (DR), false positive rates (FPR), the costs of different screening strategies for trisomy 21 and combinations of these strategies were compared. The number of fetuses with trisomy 21 at 12 + 0 weeks of gestation was estimated based on maternal age distribution. We examined the screening performance of a screening strategy based on maternal age, first trimester screening (FTS) and cffDNA testing as well as the combinations "maternal age and cffDNA" and "FTS and cffDNA". Results: In 2012 673 544 children were born. Median maternal age at delivery was 30.2 years (25th-75th quartile: 27.0-34.0). Based on maternal age distribution the expected number of fetuses with trisomy 21 at 12 weeks' gestation was 1788. Our study population therefore consisted of 675 332 pregnancies. Screening based only on maternal age or FTS or cffDNA resulted in detection rates of 63.3 %, 92.2 % and 99.0 % and false positive rates of 21.8 %, 8.0 % and 0.1 %, respectively. When maternal age was combined with cffDNA, cffDNA testing was only offered to women over a certain age; if a cut-off of 30 years was used, this resulted in a DR of 85.2 % and a FPR of 1.7 %. If primary screening consisted of FTS with cffDNA testing only done when the risk was between 1 : 10 and 1 : 1000, the detection rate was 96.7 % and the false positive rate was 1.2 %. Conclusion: In this model-based study we showed that prenatal screening for trisomy 21 can be improved even more by combining FTS and cffDNA. Further studies are necessary to examine whether these results can be reproduced in reality.
Zielsetzung: Durch die Einführung der zellfreien fetalen DNA (cffDNA)-Analyse eröffnen sich derzeit neue Möglichkeiten im pränatalen Screening auf Trisomie 21. Der höheren Testgüte stehen jedoch höhere Kosten gegenüber, sodass durch eine Kombination der verschiedenen Screening-Verfahren die Vorteile der verschiedenen Ansätze nutzbar gemacht werden sollen. In dieser Arbeit sollen die Testgüte und die Kosten der verschiedenen Screening-Ansätze untersucht werden. Methoden: In dieser Arbeit wurden in einer Modellrechnung die Detektions- und Falschpositivrate (DR und FPR) sowie die Kosten unterschiedlicher Ansätze im Screening auf Trisomie 21 und deren Kombinationen verglichen. Das Modell basierte auf den Geburten in Deutschland 2012, die den euploiden Anteil repräsentierten. Der Anteil der Feten mit Trisomie 21 bei 12 + 0 SSW wurde auf der Basis der Altersstruktur des mütterlichen Alters und deren Häufigkeit in der Geburtenkohorte 2012 geschätzt. Berechnet wurde die Testgüte für das Screening anhand des mütterlichen Alters, des Ersttrimester-Screenings, der cffDNA-Analyse sowie den Kombinationen aus mütterlichem Alter und cffDNA und ETS und cffDNA. Ergebnisse: 2012 wurden 673 544 Kinder geboren. Das mediane Alter der Mütter bei Entbindung lag bei 30,2 (25.–75. Quartil 27,0–34,0) Jahren. Entsprechend der mütterlichen Altersstruktur sind daher in der 12 + 0 SSW 1788 Feten mit Trisomie 21 zu erwarten. In Summe beinhaltet die Studienpopulation somit 675 332 Schwangerschaften. Das Screening anhand des mütterlichen Alters und des ETS resultiert in einer DR von 63,3 und 92,2 % bei einer FPR von 21,8 und 8,0 %. Für die cffDNA-Analyse werden als DR und FPR 99,0 und 0,1 % angenommen. Bei der Kombination des mütterlichen Alters und der cffDNA-Analyse wird ab einem mütterlichen Alter eine cffDNA-Analyse durchgeführt. Bei einem Schwellenwert von 30 Jahren liegen die DR und FPR bei 85,2 und 1,7 %. Bei Verwendung des ETS und im Intermediär-Risikokollektiv cffDNA sind bei Schwellenwerten von 1 : 10 und 1 : 1000 eine DR und eine FPR von 96,7 und 1,2 % zu erwarten. Schlussfolgerung: In dieser Modellrechnung konnte gezeigt werden, dass vor allem durch die Kombination aus ETS und cffDNA-Analyse das Screening auf Trisomie 21 optimiert werden kann. Nachfolgende Studien sollten untersuchen, ob die positiven Aspekte dieses Kombinationsansatzes auch in der Realität zu beobachten sind.
Keywords: cell-free fetal DNA; first trimester screening; screening; trisomy.
Conflict of interest statement
Figures
References
-
- Kagan K O, Wright D, Baker A. et al.Screening for trisomy 21 by maternal age, fetal nuchal translucency thickness, free beta-human chorionic gonadotropin and pregnancy-associated plasma protein-A. Ultrasound Obstet Gynecol. 2008;31:618–624. - PubMed
-
- Nicolaides K H. A model for a new pyramid of prenatal care based on the 11 to 13 weeksʼ assessment. Prenat Diagn. 2011;31:3–6. - PubMed
-
- Morgan S, Delbarre A, Ward P. Impact of introducing a national policy for prenatal Down syndrome screening on the diagnostic invasive procedure rate in England. Ultrasound Obstet Gynecol. 2013;41:526–529. - PubMed
-
- Kagan K O, Eiben B, Kozlowski P. Kombiniertes Ersttrimesterscreening und zellfreie fetale DNA – „Next Generation Screening“. Ultraschall Med. 2014;35:229–236. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources