

Use of Anticoagulants and Antiplatelet Agents in Stable Outpatients with Coronary Artery Disease and Atrial Fibrillation. International CLARIFY Registry
- PMID: 25915904
- PMCID: PMC4411156
- DOI: 10.1371/journal.pone.0125164
Use of Anticoagulants and Antiplatelet Agents in Stable Outpatients with Coronary Artery Disease and Atrial Fibrillation. International CLARIFY Registry
Abstract
Background: Few data are available regarding the use of antithrombotic strategies in coronary artery disease patients with atrial fibrillation (AF) in everyday practice. We sought to describe the prevalence of AF and its antithrombotic management in a contemporary population of patients with stable coronary artery disease.
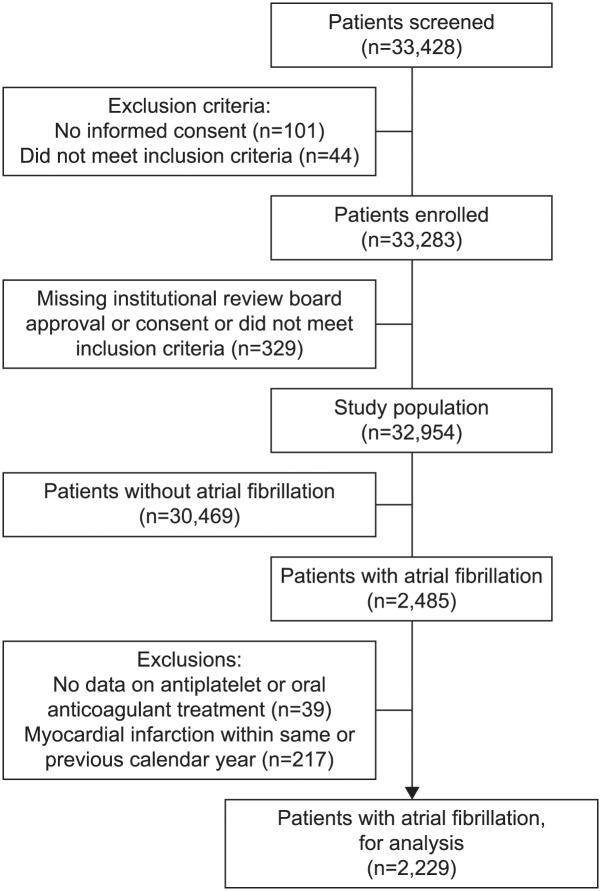
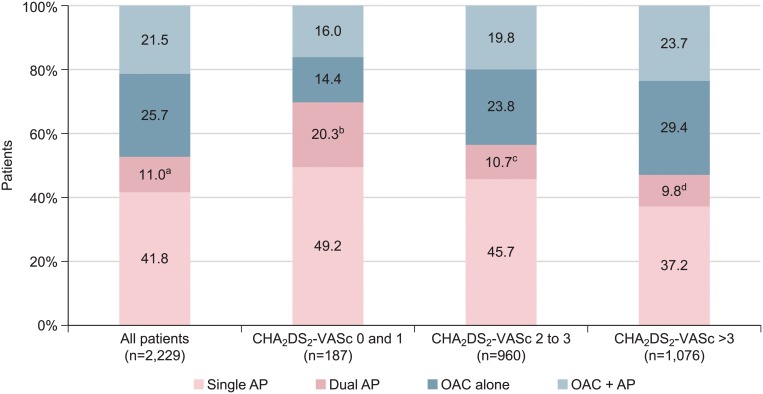
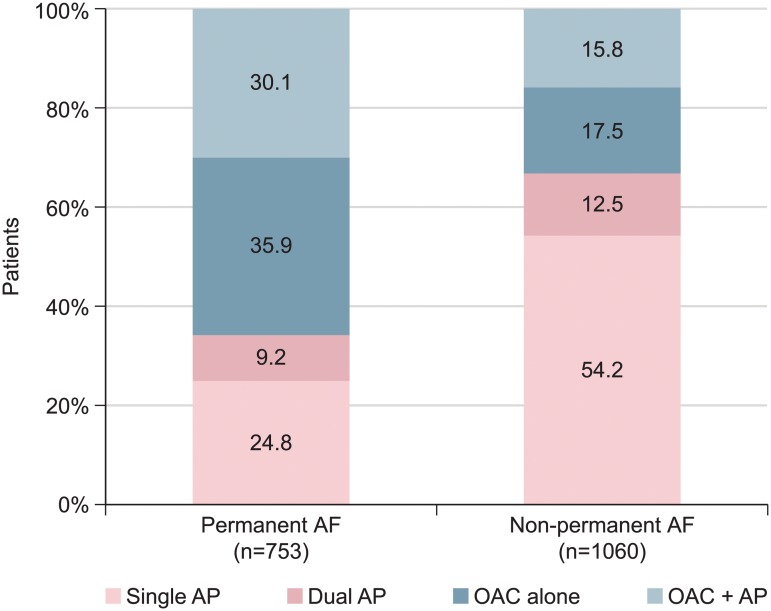
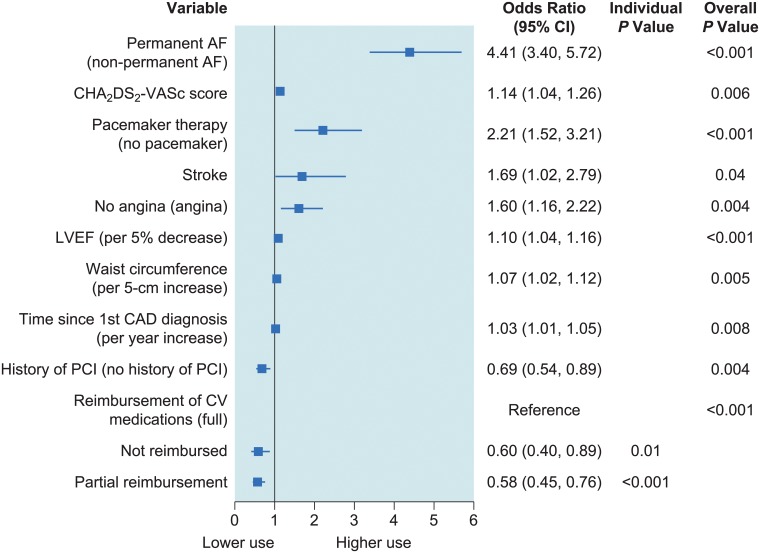
Methods and findings: CLARIFY is an international, prospective, longitudinal registry of outpatients with stable coronary artery disease, defined as prior (≥12 months) myocardial infarction, revascularization procedure, coronary stenosis >50%, or chest pain associated with evidence of myocardial ischemia. Overall, 33,428 patients were screened, of whom 32,954 had data available for analysis at baseline; of these 2,229 (6.7%) had a history of AF. Median (interquartile range) CHA2DS2-VASc score was 4 (3, 5). Oral anticoagulation alone was used in 25.7%, antiplatelet therapy alone in 52.8% (single 41.8%, dual 11.0%), and both in 21.5%. OAC use was independently associated with permanent AF (p<0.001), CHA2DS2-VASc score (p=0.006), pacemaker (p<0.001), stroke (p=0.04), absence of angina (p=0.004), decreased left ventricular ejection fraction (p<0.001), increased waist circumference (p=0.005), and longer history of coronary artery disease (p=0.008). History of percutaneous coronary intervention (p=0.004) and no/partial reimbursement for cardiovascular medication (p=0.01, p<0.001, respectively) were associated with reduced oral anticoagulant use.
Conclusions: In this contemporary cohort of patients with stable coronary artery disease and AF, most of whom are theoretical candidates for anticoagulation, oral anticoagulants were used in only 47.2%. Half of the patients received antiplatelet therapy alone and one-fifth received both antiplatelets and oral anticoagulants. Efforts are needed to improve adherence to guidelines in these patients.
Trial registration: ISRCTN registry of clinical trials: ISRCTN43070564.
Conflict of interest statement
Figures
References
-
- European Heart Rhythm Association, European Association for Cardio-Thoracic Surgery, Camm AJ, Kirchhof P, Lip GY, Schotten U, et al. Guidelines for the management of atrial fibrillation: the Task Force for the Management of Atrial Fibrillation of the European Society of Cardiology (ESC). Eur Heart J. 2010;31: 2369–2429. 10.1093/eurheartj/ehq278 - DOI - PubMed
-
- Task Force on Myocardial Revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS), European Association for Percutaneous Cardiovascular Interventions (EAPCI), Wijns W, Kolh P, Danchin N, Di Mario C, et al. Guidelines on myocardial revascularization. Eur Heart J. 2010;31: 2501–2555. 10.1093/eurheartj/ehq277 - DOI - PubMed
-
- Sorensen R, Hansen ML, Abildstrom SZ, Hvelplund A, Andersson C, Jorgensen C, et al. Risk of bleeding in patients with acute myocardial infarction treated with different combinations of aspirin, clopidogrel, and vitamin K antagonists in Denmark: a retrospective analysis of nationwide registry data. Lancet. 2009;374: 1967–1974. 10.1016/S0140-6736(09)61751-7 - DOI - PubMed
-
- Lip GY, Nieuwlaat R, Pisters R, Lane DA, Crijns HJ. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: the euro heart survey on atrial fibrillation. Chest. 2010;137: 263–272. 10.1378/chest.09-1584 - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
