

The impact of smoking on airflow limitation in subjects with history of asthma and inactive tuberculosis
- PMID: 25915938
- PMCID: PMC4411068
- DOI: 10.1371/journal.pone.0125020
The impact of smoking on airflow limitation in subjects with history of asthma and inactive tuberculosis
Abstract
Background: Although smoking is the most important and modifiable cause of chronic obstructive pulmonary disease (COPD), other risk factors including asthma and tuberculosis (TB) are also associated. It is common for COPD patients to have more than one of these risk factors. The aims of this study were to determine the prevalence of airflow limitation (FEV1/FVC<0.7) according to the risk factors and to investigate their impact and interaction in airflow limitation.
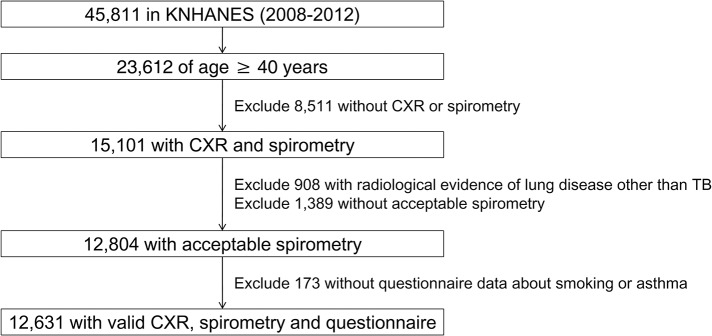
Methods: From the Korean National Health and Nutrition Examination Survey between 2008 and 2012, we analyzed participants over 40 years of age by spirometry, chest radiograph and questionnaire about asthma and smoking history.
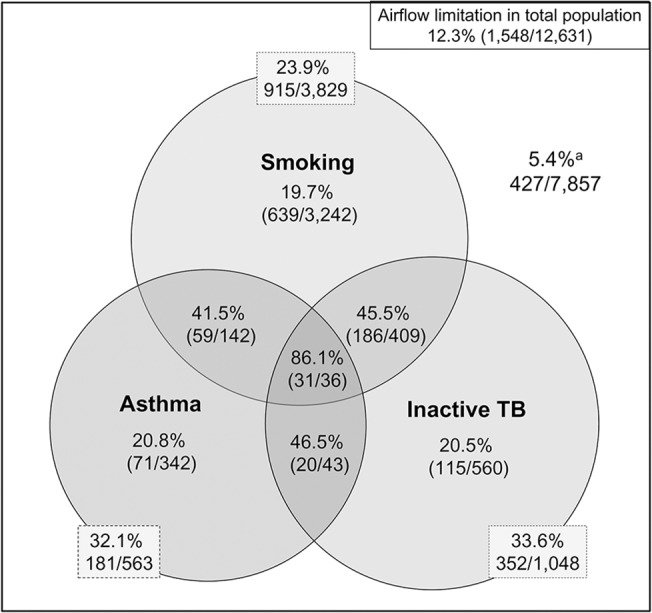
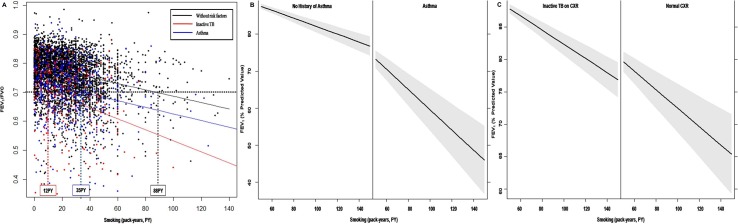
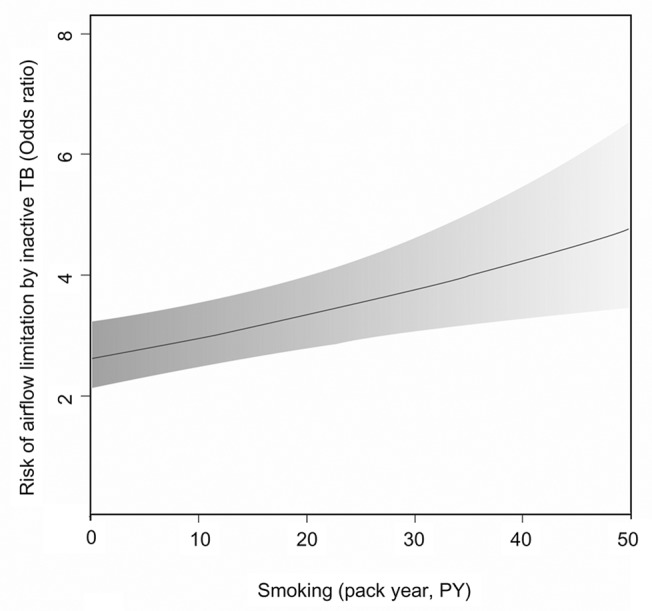
Results: Of 12,631 participants, 1,548 (12.3%) had airflow limitation. The prevalence of airflow limitation in smokers (≥10 pack-year), asthmatics, and those with inactive TB was 23.9%, 32.1%, and 33.6%. The prevalence increased with the number of risk factors: 86.1% had airflow limitation if they had all three risk factors. Impacts of inactive TB and asthma on airflow limitation were equivalent to 47 and 69 pack-years of smoking, respectively. Airflow limitation resulted from lower levels of smoking in those with inactive TB and asthma. A potential interaction between smoking and inactive tuberculosis in the development of airflow limitation was identified (p = 0.054).
Conclusions: Asthma and inactive TB lesions increase susceptibility to smoking in the development of airflow limitation. People with these risk factors should be seen as a major target population for anti-smoking campaigns to prevent COPD.
Conflict of interest statement
Figures
References
-
- Mannino DM, Buist AS (2007) Global burden of COPD: risk factors, prevalence, and future trends. Lancet 370: 765–773. - PubMed
-
- Murray CJ, Lopez AD, Black R, Mathers CD, Shibuya K, Ezzati M, et al. (2007) Global burden of disease 2005: call for collaborators. Lancet 370: 109–110. - PubMed
-
- National Herat Lung and Blood Institue (2004) Morbidity and mortality: chartbook on cardiovascular, lung, and blood diesases Bethesda: US Department of Health and Human Services. Public Health Service, National Institutes of Health.
-
- Global Institute for Chronic Obstructive Lung Disease (2013) Global strategy for diagnosis, management, and prevention of COPD. Geneva.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
