

A quantitative analysis of out-of-hospital pediatric and adolescent resuscitation quality--A report from the ROC epistry-cardiac arrest
- PMID: 25917262
- PMCID: PMC4506865
- DOI: 10.1016/j.resuscitation.2015.04.010
A quantitative analysis of out-of-hospital pediatric and adolescent resuscitation quality--A report from the ROC epistry-cardiac arrest
Abstract
Aim: High-quality cardiopulmonary resuscitation (CPR) may improve survival. The quality of CPR performed during pediatric out-of-hospital cardiac arrest (p-OHCA) is largely unknown. The main objective of this study was to describe the quality of CPR performed during p-OHCA resuscitation attempts.
Methods: Prospective observational multi-center cohort study of p-OHCA patients ≥ 1 and < 19 years of age registered in the Resuscitation Outcomes Consortium (ROC) Epistry database. The primary outcome was an a priori composite variable of compliance with American Heart Association (AHA) guidelines for both chest compression (CC) rate and CC fraction (CCF). Event compliance was defined as a case with 60% or more of its minute epochs compliant with AHA targets (rate 100-120 min(-1); depth ≥ 38 mm; and CCF ≥ 0.80). In a secondary analysis, multivariable logistic regression was used to evaluate the association between guideline compliance and return of spontaneous circulation (ROSC).
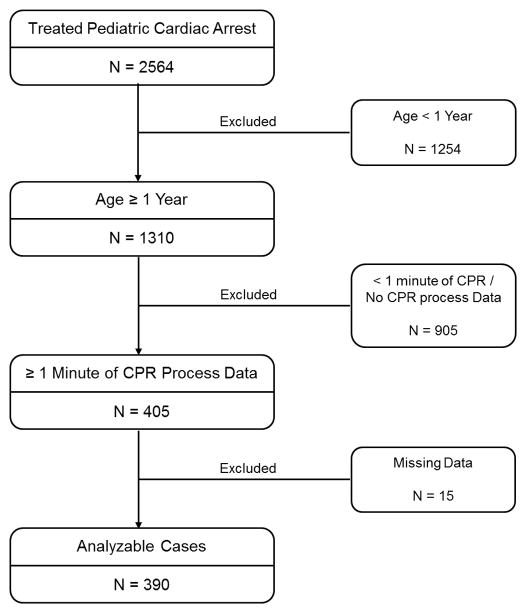
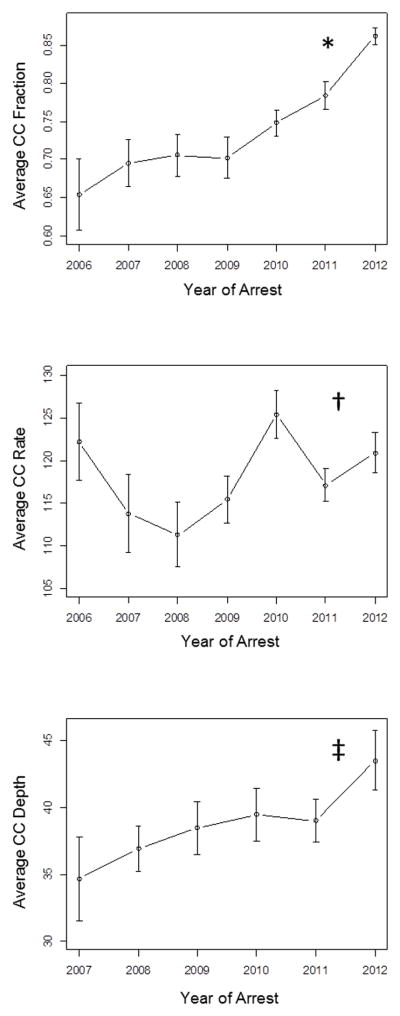
Results: Between December 2005 and December 2012, 2564 pediatric events were treated by EMS providers, 390 of which were included in the final cohort. Of these events, 22% achieved AHA compliance for both rate and CCF, 36% for rate alone, 53% for CCF alone, and 58% for depth alone. Over time, there was a significant increase in CCF (p < 0.001) and depth (p = 0.03). After controlling for potential confounders, there was no significant association between AHA guideline compliance and ROSC.
Conclusions: In this multi-center study, we have established that there are opportunities for professional rescuers to improve prehospital CPR quality. Encouragingly, CCF and depth both increased significantly over time.
Keywords: Cardiopulmonary resuscitation; Emergency medical services; Pediatric.
Copyright © 2015 Elsevier Ireland Ltd. All rights reserved.
Conflict of interest statement
Dr. Robert M. Sutton receives funding from the National Institute of Child Health and Human Development (NICHD; K23HD062629) and has received a speaker honoraria from Zoll Medical. Dr. Christian Vaillancourt is supported by a University of Ottawa Research Chair. He has received funding from the Canadian Institutes of Health Research, the Heart and Stroke Foundation of Canada, and the National Institutes of Health (NIH) for work related to cardiac arrest and prehospital care. Dr. Mohamud Daya receives funding from the NIH and is an unpaid consultant for Philips HealthCare. Dr. Sheldon Cheskes receives grant funding from the NIH as co-primary investigator (PI) of the ROC Toronto site. He has received speaker honoraria and funding from Zoll Medical. Dr. Ahamed H. Idris receives research funding from the National Heart, Lung, and Blood Institute (NHLBI), the US Army, and the AHA. Dr. James J. Menegazzi receives funding from the NHLBI (R01HL117979). Dr. Graham Nichol has received support from the NIH as co-PI of the ROC Coordinating Center. He is the PI of the Dynamic AED Registry which is funded by the Food and Drug Administration, Cardiac Science Corporation, Heartsine Technologies Inc., Philips Healthcare Inc., Physio-Control Inc., and the Zoll Medical Corporation. He is PI of the Simple EMS Registry funded by the AHA, and PI of the Washington Study of Ultrasound in Resuscitation funded by Philips Healthcare Inc. Erin Case, Jack Nuttall, Heather Herren, and Drs. Ian R. Drennan, Michael A. Austin, Siobhan P. Brown, Clifton W. Callaway, Douglas L. Andrusiek, Jim Christenson, Diane L. Atkins, Vinay M. Nadkarni, Jonathan Kaltman, Jamie Hutchison, Thomas D. Rea, and Robert A. Berg have nothing to disclose.
Figures
References
-
- Kitamura T, Iwami T, Kawamura T, et al. Nationwide improvements in survival from out-of-hospital cardiac arrest in japan. Circulation. 2012;126(24):2834–2843. - PubMed
-
- Donoghue AJ, Nadkarni V, Berg RA, et al. Out-of-hospital pediatric cardiac arrest: An epidemiologic review and assessment of current knowledge.[see comment] Ann Emerg Med. 2005;46(6):512–522. - PubMed
Publication types
MeSH terms
Grants and funding
- NIH U01 HL077863-05/HL/NHLBI NIH HHS/United States
- U01 HL077866/HL/NHLBI NIH HHS/United States
- U01 HL077871/HL/NHLBI NIH HHS/United States
- K23 HD062629/HD/NICHD NIH HHS/United States
- R01 HL117979/HL/NHLBI NIH HHS/United States
- HL077867/HL/NHLBI NIH HHS/United States
- 5U01 HL077863/HL/NHLBI NIH HHS/United States
- L40 HD070138/HD/NICHD NIH HHS/United States
- HL077887/HL/NHLBI NIH HHS/United States
- U01 HL077881/HL/NHLBI NIH HHS/United States
- R01HL117979/HL/NHLBI NIH HHS/United States
- HL077873/HL/NHLBI NIH HHS/United States
- HL077871/HL/NHLBI NIH HHS/United States
- HL077881/HL/NHLBI NIH HHS/United States
- HL077908/HL/NHLBI NIH HHS/United States
- K23HD062629/HD/NICHD NIH HHS/United States
- U01 HL077887/HL/NHLBI NIH HHS/United States
- U01 HL077885/HL/NHLBI NIH HHS/United States
- CAPMC/ CIHR/Canada
- U01 HL077865/HL/NHLBI NIH HHS/United States
- U01 HL077863/HL/NHLBI NIH HHS/United States
- U01 HL077908/HL/NHLBI NIH HHS/United States
- HL077872/HL/NHLBI NIH HHS/United States
- HL077866/HL/NHLBI NIH HHS/United States
- U01 HL077873/HL/NHLBI NIH HHS/United States
- U01 HL077867/HL/NHLBI NIH HHS/United States
- HL077885/HL/NHLBI NIH HHS/United States
- HL077865/HL/NHLBI NIH HHS/United States
- U01 HL077872/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
