

Follicular dendritic cell sarcoma of the head and neck: Case report, literature review, and pooled analysis of 97 cases
- PMID: 25917851
- PMCID: PMC4696909
- DOI: 10.1002/hed.24115
Follicular dendritic cell sarcoma of the head and neck: Case report, literature review, and pooled analysis of 97 cases
Abstract
Background: Follicular dendritic cell sarcoma (FDCS) is a rare lymphoid neoplasm presenting in the head and neck. There are no pooled analyses of head and neck FDCS cases in the English language literature.
Methods: A MEDLINE and PubMed review of cases from 1978 to February 2014 was performed. Demographics, clinicopathologic data, and outcomes were summarized.
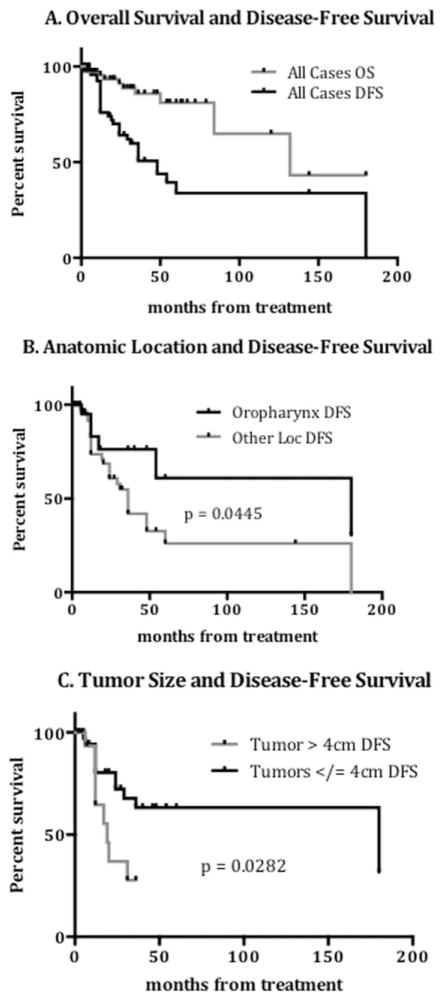
Results: We presented 2 patients and analyzed 97 cases. The mean age was 42.7 years (SD = 16.3 years). Outcomes were available for 76 patients. Tumors ≤4 cm had better disease-free survival (63% vs 28% at 5 years; p = .0282). Locoregional recurrence was significantly less likely with surgery and radiation compared to surgery alone (15% vs 45%; p = .019) and in patients receiving a neck dissection (10% vs 43%; p = .046).
Conclusion: This pooled analysis provides the largest sample size of FDCS of the head and neck to date and suggests that radiation and neck dissection may be beneficial to locoregional oncologic control. © 2015 Wiley Periodicals, Inc. Head Neck 38: E2241-E2249, 2016.
Keywords: dendritic cell; follicular dendritic cell sarcoma (FDCS); head and neck; sarcoma.
© 2015 Wiley Periodicals, Inc.
Figures
References
-
- Saygin C, Uzunaslan D, Ozguroglu M, Senocak M, Tuzuner N. Dendritic cell sarcoma: a pooled analysis including 462 cases with presentation of our case series. Crit Rev Oncol Hematol. 2013;88:253–271. - PubMed
-
- Fonseca R, Yamakawa M, Nakamura S, et al. Follicular dendritic cell sarcoma and interdigitating reticulum cell sarcoma: a review. Am J Hematol. 1998;59:161–167. - PubMed
-
- Chan JK, Fletcher CD, Nayler SJ, Cooper K. Follicular dendritic cell sarcoma. Clinicopathologic analysis of 17 cases suggesting a malignant potential higher than currently recognized. Cancer. 1997;79:294–313. - PubMed
-
- Perkins SM, Shinohara ET. Interdigitating and follicular dendritic cell sarcomas: a SEER analysis. Am J Clin Oncol. 2013;36:395–398. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
