

Multidrug-Resistant Tuberculosis and Extensively Drug-Resistant Tuberculosis
- PMID: 25918181
- PMCID: PMC4561400
- DOI: 10.1101/cshperspect.a017863
Multidrug-Resistant Tuberculosis and Extensively Drug-Resistant Tuberculosis
Abstract
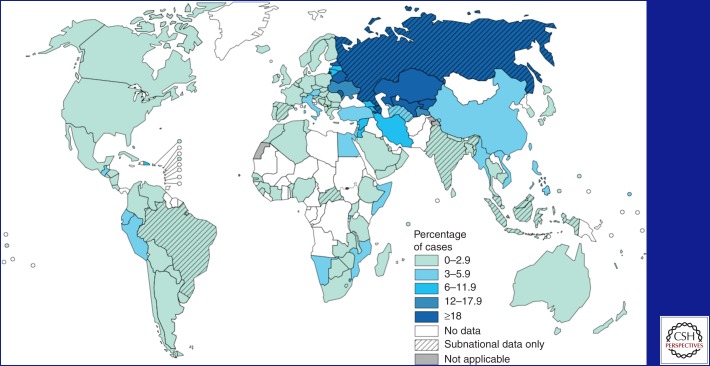
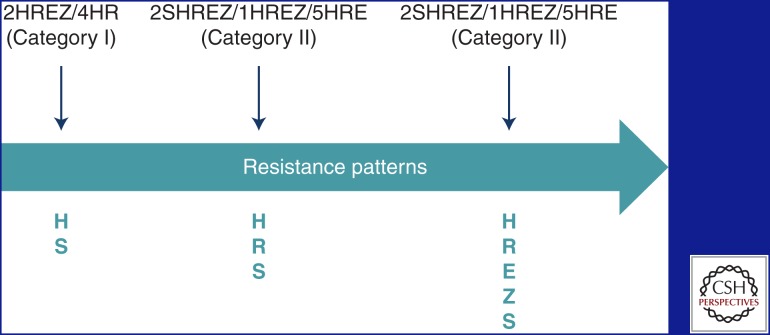
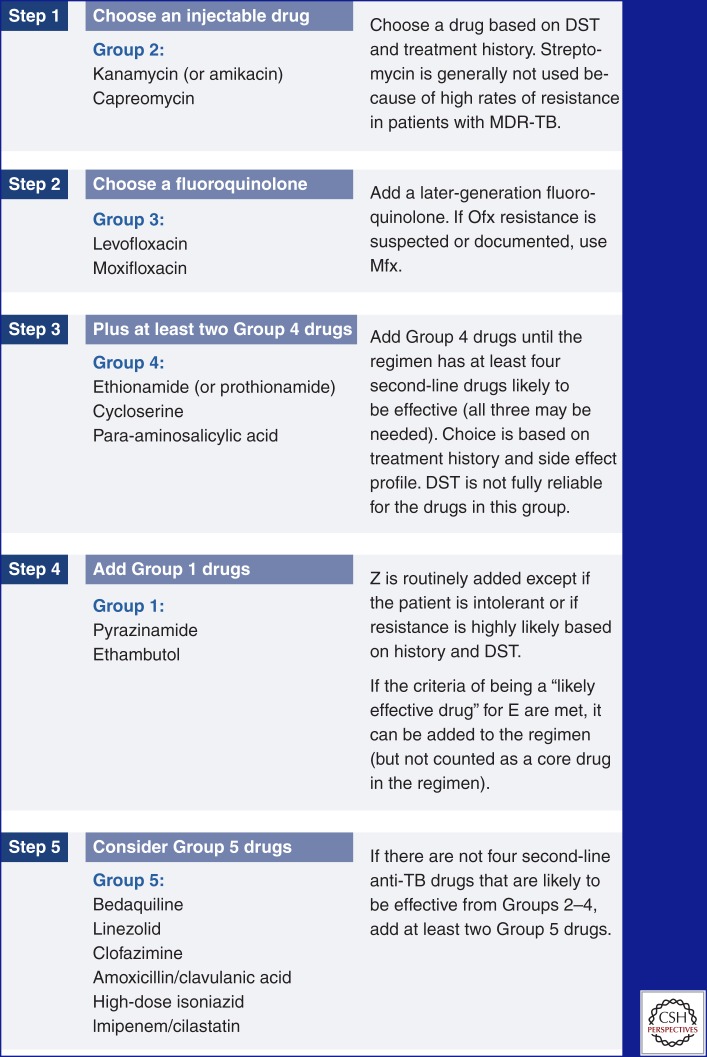
The continuing spread of drug-resistant tuberculosis (TB) is one of the most urgent and difficult challenges facing global TB control. Patients who are infected with strains resistant to isoniazid and rifampicin, called multidrug-resistant (MDR) TB, are practically incurable by standard first-line treatment. In 2012, there were approximately 450,000 new cases and 170,000 deaths because of MDR-TB. Extensively drug-resistant (XDR) TB refers to MDR-TB strains that are resistant to fluoroquinolones and second-line injectable drugs. The main causes of the spread of resistant TB are weak medical systems, amplification of resistance patterns through incorrect treatment, and transmission in communities and facilities. Although patients harboring MDR and XDR strains present a formidable challenge for treatment, cure is often possible with early identification of resistance and use of a properly designed regimen. Community-based programs can improve treatment outcomes by allowing patients to be treated in their homes and addressing socioeconomic barriers to adherence.
Copyright © 2015 Cold Spring Harbor Laboratory Press; all rights reserved.
Figures
References
-
- Ahuja SD, Ashkin D, Avendano M, Banerjee R, Bauer M, Bayona J, Becerra M, Benedetti A, Burgos M, Centis R, et al. 2012. Multidrug resistant pulmonary tuberculosis treatment regimens and patient outcomes: An individual patient data meta-analysis of 9,153 patients. PLoS Med 9: e1001300. - PMC - PubMed
-
- Becerra M, Franke MF, Appleton SC, Joseph JK, Bayona J, Atwood SS, Mitnick CD. 2013. Tuberculosis in children exposed at home to multidrug-resistant tuberculosis. Pediatr Infect Dis J 32: 115–119. - PubMed
-
- Cegielski JP. 2010. Extensively drug-resistant tuberculosis: “There must be some kind of way out of here”. Clin Infect Dis 50: S195–S200. - PubMed
-
- Centers for Disease Control and Prevention (CDC). 2013. Provisional CDC guidelines for the use and safety monitoring of bedaquiline fumarate (Sirturo) for the treatment of multidrug-resistant tuberculosis. MMWR Recomm Rep 62: 1–12. - PubMed
-
- Chavez Pachas AM, Blank R, Fawzi Smith MC, Bayona J, Becerra M, Mitnick CD. 2004. Identifying early treatment failure on category I therapy for pulmonary tuberculosis in Lima Ciudad, Peru. Int J Tuberc Lung Dis 8: 52–58. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical